ECONOMIC INEQUALITY AS A DETERMINANT OF HEALTH
17.5.1 Overview
More than 20 years ago, Wilkinson (1990, 1992) introduced the hypothesis that income inequality is harmful to health. He showed that countries with higher-income inequality have lower life expectancy, and others soon confirmed a negative association with other measures of population health (Steckel, 1995; Waldmann, 1992).
According to one variant of the hypothesis, this cross-country association reflects a causal effect of income inequality on individual health via psychosocial mechanisms: striving to keep up with the Joneses in societies with higher levels of income inequality raises levels of stress. Income redistribution can potentially raise average health not only because of any greater responsiveness of health to income at lower levels of income, if indeed there is a causal effect of income on health, but also because narrower disparities in income are good for everyone’s health, including that of the rich.The validity of this hypothesis has been heavily debated (Gravelle, 1998; Smith, 1999; Wilkinson and Pickett, 2006), and associated claims that economic inequality is responsible for a host of societal ills beyond poor health, including violence, teenage pregnancy, obesity, mistrust, and high incarceration rates (Wilkinson and Pickett, 2010), has attracted much attention and been subject to a good deal of criticism (Saunders and Evans, 2010; Snowdon, 2010). In the present context, establishing whether there is a health cost of economic inequality is relevant to the evaluation of the strength of an instrumental argument for reducing inequality.
We focus here on the mechanisms through which income inequality can potentially impact health, and we pay close attention to whether empirical analyses are capable of testing the hypotheses. We restrict our attention to the impact of inequality on morbidity and mortality, and we neglect studies of homicides, for which there is general agreement on the importance of income inequality (Deaton, 2003; Lynch et al., 2004b).
We also steer clear of the happiness literature that has paid a great deal of attention to income inequality (Alesina et al., 2004; Clark et al., 2008).In the next subsection, we demonstrate the stylized fact that population health is negatively associated with income inequality, and we outline the mechanisms through which income inequality might threaten the health of all individuals. We then consider alternative theories that can explain the negative association between population health and income inequality at the aggregate level without inequality being a threat to the health of all individuals in a society. We then turn to the evidence.
17.5.2 Basic Hypothesis: InequalityThreatens Everyone's Health
Population health rises with per capita income but at a decreasing rate (Preston, 1975). Among high-income countries, where this so-called Preston curve flattens out, population health has been found to be negatively correlated with income inequality (Wilkinson, 1992, 1996; Wilkinson and Pickett, 2010). There is only weak evidence of this in Figure 17.5, which is based on the same data on life expectancy, as well as measures of inequality employed in a popular publication that advances the inequality hypothesis (Wilkinson and Pickett, 2010). In these data, the relationship appears to be driven by the low inequality and high life expectancy of Japan and Sweden, and the high inequality and low life expectancy of the USA and Portugal. Among the bulk of countries with life expectancies of 78—80 years, there appears to be no relationship with income inequality.[105]
A negative correlation between income inequality and average health, presuming it exists, has been attributed to the falling potency of further, material gains in generating health once the average standard of living reaches a threshold beyond which income differences become more relevant to the determination of health (Wilkinson and Pickett, 201 0).[106] Two causal mechanisms through which income inequality may threaten the
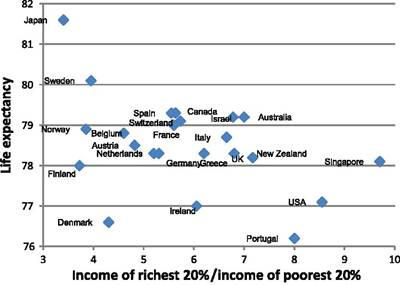
Figure 17.5 Life expectancy and income inequality in high-income countries.
Notes: Data are from Wilkinson and Pickett (2010) who, in turn, took them from UN Human Development Reports. Life expectancy is at birth averaged over males and females in 2004. Income inequality is measured by the ratio of income received by the richest 20% of households to the income of the poorest 20% averaged over the years 2003-2006.health of all individuals—rich and poor—have been proposed. The first stresses the importance of the public provision of health-determining goods, while the second focuses on social capital. Some stress a third psychosocial mechanism mentioned above (Wilkinson, 1992). Given that this theory does not propose that income inequality affects health throughout the distribution of income, but rather that the health of less well-off individuals suffers because of their relative deprivation, we cover this assertion in the next section.
The public provision of goods would create a pathway from income inequality to individual health if inequality impacts on the provision of goods that determine health, such as curative and preventive health care, education, and sanitation. Income inequality might lead to more heterogeneous preferences, which will reduce the average value (and thus the provision) of publicly provided goods (Alesina et al., 1999; Deaton, 2003; Thorbecke and Charumilind, 2002). But income inequality could also lead to increased public provision because a more skewed income distribution will reduce the income of the median voter relative to the mean and increase the redistributive effect of public provisions financed by nonregressive taxation (Meltzer and Richard, 1981). Following Sen (1999), Deaton (2003, forthcoming) argues that the focus should be on the health consequences of political, rather than economic, inequalities. He notes that in nineteenth-century Britain, and in the USA and India in the twentieth century, substantial improvements in public health were realized after the extension of political rights.
Social capital—cohesion and trust among citizens (Putnam et al., 1993)—is argued to be a consequence of economic inequality and a determinant of health via social and psychosocial support, informal insurance mechanisms, and information diffusion (d’Hombres et al., 2010; Kawachi and Kennedy, 1997; Kennedy et al., 1998; Ronconi
et al., 2012).
This hypothesis has received a fair amount of attention in the literature, but whether this attention is justified depends on the assumption that income inequality reduces social cohesion, as opposed to lower social cohesion raising income inequality, which is an equally plausible explanation.17.5.3 Alternative Hypotheses: Health Responds to Absolute or Relative Income
A negative association between population health and income inequality could arise from the dependence of health on absolute or relative income, without this necessarily implying that inequality threatens everyone’s health (Wagstaff and van Doorslaer, 2000). The absolute income hypothesis states that diminishing health returns to income at the individual health level explain the negative association between average population health and income inequality at the aggregate level (Gravelle, 1998; Gravelle et al., 2002; Rodgers, 1979; Wildman et al., 2003). Ifthe health-income relationship is concave then an increase in the spread of the income distribution will bring down mean health because the health loss to those becoming poorer is larger than the health gain to those becoming richer. Income redistribution could raise average population health but this would occur without the health of any individual, given his or her income, being directly affected by the level of economic inequality in society. The literature reviewed in Section 17.4 provides only limited evidence of a causal impact of income on health in high-income countries, but some evidence indicates that the effect is stronger among the poor, and there does appear to be an income effect in low-income countries. If there are health returns to income, they would appear to be diminishing. But even if there is no (diminishing) causal effect of income on health, a negative statistical association between average health and income inequality will be observed when there is a concave statistical relationship between health and income across individuals.
According to the relative income hypothesis, one’s health depends on how one’s income fares relative to others. When there are diminishing health returns to the difference between individual income and some aggregate, such as the mean, there will be a negative association between average health and income inequality. These hypotheses are distinguished—unfortunately, often not explicitly—from the above-mentioned income inequality hypothesis by the assertion that income inequality only matters to the extent that it increases the number of individuals who have an income deficit relative to some reference level. It is only the health of these individuals that is claimed to be damaged by inequality. In contrast, the income inequality hypothesis postulates that income inequality is a common factor impacting on the health of everyone.
Health is presumed to depend on relative income because of psychosocial effects. It is not so much possession of more material goods that matters for health, but rather the stress, depression, anxiety, shame, and distrust brought on by judging one’s standard of living to fall short of that enjoyed by others. These emotional responses are claimed to trigger health-damaging psychoneuroendocrine reactions, such as increased cortisol production (Wilkinson, 1992). Some have even hypothesized that this psychosocial- biological effect may be hardwired into humans through our evolutionary experience (Wilkinson, 2001). Hunter-gatherer societies were extremely egalitarian, and humans might not yet be well adapted to the social inequalities that have arisen in settlement societies. Consistent with the psychosocial-biological mechanism, experiments have found that manipulating baboons, which also have stable, although obviously much simpler, hierarchical societies, into lower social positions induces stress (Sapolsky, 2005). It has been hypothesized that low relative economic status may impact negatively on health through epigenetic responses, as well (Wilkinson and Pickett, 201 0).[107] Wilkinson and Pickett cite evidence of the maternal nursing behavior of rats affecting the offspring’s epigenome at a (glucocortoid) receptor known to regulate stress responses (Weaver et al., 2004).
They propose that, if this also occurs among humans, then increased stress and cortisol levels experienced throughout life could be due to early-life epigenetic processes. These authors do not elaborate on why exposure to such processes may be related to low (parental) socioeconomic position, although there is evidence of associations between epigenetic differences and SES, which is proxied by income position, occupation, education, and housing tenure among adults (McGuinness et al., 2012) and children (Borghol et al., 2012). Understanding of the epidemiological implications of epigenetic processes is still limited (Relton and Davey Smith, 2012), and it would certainly be premature to presume that they contribute to health differences across socioeconomic environments.Why psychosocial responses should be confined to inequality in the income dimension has been questioned (Deaton, 2003, 2013). It seems quite conceivable that they might be triggered, perhaps more strongly so, by comparisons of occupation, education, housing, and so on. While describing the mechanism in the previous paragraphs, we (and the authors cited) have often resorted to terms such as social hierarchy. The most influential research on health and social position—the Whitehall studies (Marmot et al., 1978, 1991)—has used occupational grade as the discriminating indicator. The evidence obtained from animal studies cannot, of course, inform us about effects in the income dimension. In reviewing the evidence below, we focus on the health effects of relative income, but this is because ofthe context of this chapter and not because we believe other dimensions of SES to be of lesser importance to health.
Less frequently cited than the psychosocial mechanism is the idea that pecuniary externalities, arising from the pricing of health-enhancing goods, reduce average health in regions that are more unequal (Miller and Paxson, 2006). Take the case of healthy foods. When the quality and availability of healthy food is comparable across regions, but more expensive in rich areas, then poor individuals in these areas will have worse health than their equivalents in poorer areas. Health depends negatively on the individual’s income deficit from the regional average because of the price effect on the cost of maintaining health. But there could be an offsetting effect through collectively and locally financed health-enhancing goods, which may include some medical care. The larger tax base of wealthier neighborhoods will increase the supply and quality of health care, which will raise the health of a poor person in the rich region compared with his equivalent in a poor region.
There are three variants of the relative hypothesis—relative income, relative deprivation, and relative position—distinguished (again, often not explicitly) by the functional form linking health to income differences (Wagstaff and van Doorslaer, 2000). The relative income hypothesis proposes that the magnitude of the difference between income and that of a reference group is what ultimately matters for health (Deaton, 2001a,b, 2003; Deaton and Paxson, 2004). The average income of the group is mostly used as the point of reference, but other aggregations seem equally plausible, and there is no theoretical guidance on this. The reference group is likely to be unobservable or, at best, observed with error, and this will lead to income inequality reentering the picture even when it exerts no causal effect on individual health (Deaton, 2001b, 2003). The relative deprivation hypothesis posits that health is responsive to the difference between income and all larger incomes within the same reference group (Deaton, 2001b; Eibner and Evans, 2005; Yitzhaki, 19 79).[108] Lower incomes are assumed to be irrelevant for health, and so the point of reference is individual-specific. The relative position hypothesis suggests that the magnitude of income differences is unimportant and that health responds only to rank in the income distribution. This hypothesis is closest to the aforementioned theories that stress the importance of social hierarchy. It might also be used to justify choice of a rank-based measure of income-related health inequality, such as the concentration index (Wagstaffet al., 1991).
17.5.4 Evidence
17.5.4.1 EmpiricalChallenges
Tests have been performed using data at three levels of aggregation: country, region, and individual. The majority of studies, and most of the early ones, have relied on countrylevel data, although early US studies used state-level data. Individual-level data is required to discriminate between the five hypotheses (income inequality, absolute income, relative income, relative deprivation, and relative position) because income inequality will
correlate with average population health under all of them (Deaton, 2003; Lynch et al., 2004b; Mackenbach, 2002; Wagstaff and van Doorslaer, 2000).
The relative hypotheses provoke many unanswered questions with respect to the reference groups: how are they formed, does each individual have a unique reference, and how are they to be defined in the data? Testing is further complicated by the potential for position in relation to the reference to be endogenous through choices of group membership. Data quality and the reliability of measures of income inequality are other major issues (Deaton, 2003; West, 1997). Estimates of income inequality or relative income at town or village levels may be derived from relatively few observations and so lack precision (Leigh et al., 2009).
A major problem for analyses identifying effects from cross-country or regional variation is that time-invariant unobservable determinants of health may be correlated with income inequality. Fixed effects methods are unlikely to prove successful at aggregated levels because income inequality tends to evolve rather slowly, and measurement error bias is compounded (Babones, 2008). In addition, fixed effect estimators only identify short run effects and may fail to detect inequality effects operating with a lag. Reverse causality is unlikely to be a major problem at more aggregated levels, but through one or more of the mechanisms identified in Section 17.3, relative income could certainly be a function of health. This would tend to induce bias toward concluding that low relative income exerts a negative impact on health. These limitations must be kept in mind in interpreting the evidence.
We differentiate the evidence by the nature of the hypothesis tested and the level of data aggregation. Given that the impact of income on health is covered in Section 17.4, we do not explicitly consider evidence for the absolute income hypothesis, although we do note what happens to the health-income inequality relationship when individual income is controlled for. Studies published since previous reviews and a few key earlier papers are summarized in Tables 17.8-17.10.
17.5.4.2 Income Inequality Hypothesis
Previous reviews have concluded that the evidence does not point to income inequality as an important determinant of individual health, and this seems to hold for both morbidity and mortality (Deaton, 2003; Leigh et al., 2009; Lynch et al., 2004b; Subramanian and Kawachi, 2004; Wagstaff and van Doorslaer, 2000). They also infer from the literature that state-level income inequality associates negatively with health in the USA, but this is not true in other countries, and this difference most likely reflects racial composition at the state level, although this interpretation is disputed (Subramanian and Kawachi, 2004). There is agreement on the importance of appropriately defining
Wilkinson and Pickett, 2006 dissent, referring mainly to studies using country-level or state-level analyses to infer that income inequality is important for health.
Table 17.8 Cross-country evidence on population health-income inequality association
| Authors | CountriesZregion and period | Data | Estimator | (Partial) correlation with income inequality |
| Pascual | 12 EU countries | ECHP and | Linear RE | LE -, U5MR + |
| et al. (2005) | 1994-2001 | OECD | and FE | |
| Cantarero | 12 EU countries | ECHP and | Linear RE | LE -, U5MR + |
| et al. (2005) | 1994-2001 | OECD | and FE | |
| Babones | 134 countries | WIID and | OLS, FD | LE -, IMR +, |
| (2008) | 1970-1995 | World Bank | murder rate ns | |
| Biggs et al. | 22 Latin American | WDID, GTD, | Linear FE | LE ns, IMR ns |
| (2010) | countries 1960-2007 | WIID, SEDLAC | ||
| Wilkinson | 25 rich income | UNHDR, | Bivariate | LE -, IMR +, |
| and Pickett | countries 2000, 2001, | WDID, IOT, | association | mental health —, |
| (2010) | 2002, 2003, 2004 | WHO | obesity + | |
| Regidor | 21 OECD countries | OECD | Bivariate | 1995 IMR +, |
| etal. (2012) | 1995, 2000, 2005 | association | 2005 IMR ns | |
| Avendano | 34 OECD countries | WIID, OECD | Poisson FE | IMR ns |
| (2012) | 1960-2008 | |||
| Tacke and | 93 countries | WIID, | OLS | LE -, IMR +, |
| Waldmann (2013) | 1999-2005 | WDID, GHN | U5MR + |
Notes: LE — indicates that life expectancy is negatively correlated with income inequality. IMR + indicates the infant mortality is positively correlated with income inequality. Acronyms of other health indicators, datasets, and estimators are explained in Table A2. ns indicates no significant association.
reference groups: when references are defined with respect to smaller geographic units, such as towns or cities, there is less evidence of an association between income inequality and health.
17.5.4.2.1 Cross-Country Data
The positive cross-country association between mortality and income inequality is well documented and has been confirmed for 12 European countries (Cantarero et al., 2005; Pascual et al., 2005), 25 high-income countries (Wilkinson and Pickett, 2010), and across many countries worldwide (Babones, 2008; Tacke and Waldmann, 2013) (Table 17.8). But the positive association between infant mortality and income inequality across OECD countries evident in 1995 was no longer apparent in 2005 data (Regidor et al., 2012). It also appears that the relationship between population health and income inequality is reversed across low-income countries (Nilsson and Bergh, 2013).
Table 17.9 US cross-region evidence of population health-income inequality association
| Authors | Regional unit and period | Data | Estimator | Health measure | (Partial) correlation with income inequality |
| Ash and | 287 MSA | CMF, STF | WLS | Age- | Varies with size of |
| Robinson | 1990 | adjusted | MSA | ||
| (2009) | mortality ratio | ||||
| Deaton | 287 MSA | CMF, PUMS | WLS | Age- | No robust |
| and | 1980, 1990 | adjusted | association | ||
| Lubotsky | mortality | (conditional on | |||
| (2009) | ratio | racial composition) | |||
| Wilkinson | 50 states | Census and | Bivariate | LE, infant | LE -, IMR +, |
| and Pickett | 1999-2002 | CHS, | association | deaths, | obesity + |
| (2010) | NHANES, BRFSS | obesity | |||
| Yang et al. | 3072 | CMF | QR | Age- | + with effect |
| (2012) | counties | adjusted | increasing in | ||
| 1998-2002 | mortality | magnitude until | |||
| ratio | 80th percentile of mortality |
Notes: —/+ indicates negative/positive association of health indicator with income inequality. See Table A2 for explanation of acronyms. MSA is Metropolitan Statistical Area.
The association between population health, measured by life expectancy or infant mortality, and income inequality that is observed across countries is not evident in time variation within countries, even when exploiting very long time series. For example, there is no association between income inequality and mortality between 1900 and 1998 in the USA (Lynch et al., 2004a). Data for Australia, Canada, New Zealand, the USA, and eight European countries display no associations between the within- country evolution of either life expectancy or infant mortality and the income share of the richest 10% (contemporaneous and lagged) between 1903 and 2003 (Leigh and Jencks, 2007). There is also no relationship in the data for 22 Latin American countries between 1960 and 2007 (Biggs et al., 2010). There is an association between the change in income inequality, on the one hand, and the change in life expectancy or infant mortality, on the other hand, for over 90 countries between 1975 and 1995, but this disappears when the change in GDP per capita is controlled for (Babones, 2008). Finally, Avendano (2012) finds no association between within-country variation in infant mortality and income inequality over 4 decades for 34 OECD countries. This finding remains unchanged after allowing for country-specific (linear) time trends or allowing for a lag of 15 years between changes in income inequality and changes in infant mortality.
Table 17.10 Individual-level evidence of association between health and income, relative income,and income inequality
Country, region,
| Authors | period | Data | Estimator | Findings |
| Gerdtham and | Sweden, 284 | ULF, NCD, | Cox | 10-17 yr. survival: + |
| Johannesson (2004) | municipalities 1980-1986 | and NITS register data | proportional hazard | AI, ns RI, ns INEQ |
| Li and Zhu (2006) | China 180 communities 1993 | CHNS | Probit | Excellent/good SAH: + AI, ns RD, ns RP, ∩ INEQ Physical conditions: ~AI, ns RD, ns RP, - INEQ (physical conditions = ADL) |
| Jones and Wildman (2008) | UK 1991-2001 | BHPS | OLS, FE, RE | Good SAH: + AI, ns RD GHQ: - AI, - RD |
| Lorgelly and Lindley (2008) | UK 19 regions 1991-2002 | BHPS | Pooled, RE, and Mundlak ordered probit | Better SAH: + AI, ns RI, ns INEQ |
| Petrou and Kupek (2008) | UK 2003 | HSE | WLS | EQ-5D: + SC |
| Gravelle and Sutton (2009) | UK 11 areas 1979-2000 | GHS | Pooled binary and ordered probit | Better SAH: + AI, - RI, - INEQ Long-term illness: - AI, - RI; - INEQ |
| Hildebrand and Kerm (2009) | 11 EU countries, 52 EU regions 1994-2001 | ECHP | Linear FE | better SAH: ~ AI, - RI, - INEQ (effect size negligible) |
| Theodossiou and Zangelidis (2009) | 6 EU countries 2004 | SOCIOLD | Linear IV | Worse ADL: - AI, + RD Better SAH: + AI, ns RD Mental health: + AI, - RD |
| d’Hombres et al. (2010) | 8 former Soviet countries 2001 | LLH | Probit, OLS, GMM | Better SAH: + SC |
| Karlsson et al. (2010) | 21 low-/ middle-∕high- income countries | FORS, WIID | Pooled ordered probit | Better SAH: + AI, + RI, - INEQ in rich countries (= better ADL) |
Table17.10 Individual-Ievelevidenceofassociation between healthandincome,relativeincome,and income inequality—cont'd
Country, region,
| period | Data | Estimator | Findings | |
| Mangyo and Park (2011) | China 2004 | CIDJ | OLS | Better SAH: + RI, - RD, + RP (= mental health) |
| van Groezen et al. (2011) | 10 EU 2004 | SHARE | OLS | Better SAH: + SC |
| Fang and Rizzo (2012) | China 54 cities and counties 1997-2006 | CHNS | FE logit | Better SAH: - INEQ (effect size larger for poorer) |
| Gronqvist et al. (2012) | Sweden municipalities 1987-2004 | Hospital admissions register | Linear FE | Hospital admission: ns INEQ (= sickness leave and mortality) Better SAH: - INEQ |
| Lillard et al. (2012) | Australia, Germany, UK, USA | CNEF | Ordered probit | |
| Ronconi et al. (2012) | Argentina 1997 | Encuesta de Desarrollo Social | Bivariate probit | Better SAH: + SC |
| Nilsson and Bergh (2013) | Zambia 155 constituencies, 72 districts, 9 provinces 2004 | LCMS IV | OLS and 2SLS | HAZ: + AI, - RI (constituency reference), + RI (provincial reference), + INEQ |
Notes: AI, absolute income; RI, relative income; INEQ, income inequality; RD, relative deprivation; RP, relative position; SC, social capital. Read “XXX: AI+” as the health indicator XXX is significantly positively associated with absolute income. Same for RI, INEQ, RD, RP, and SC. Similarly: — indicates negative association; ns indicates no significant association; ~ AI indicates no consistent evidence in favor of or against AI hypothesis (respectively for INEQ, RI, RD, RP, and SC hypotheses); ∩ INEQ indicates an inverse U shape relationship with income inequality. When indicated in the second column, regional unit indicates the level at which income inequality and references for relativities are defined. When not indicated inequality/relativities is at national level. See Table A2 for explanation ofother acronyms.
The absence of any evidence that population health moves with changes in income inequality strongly suggests that the static cross-country relationship does not derive from a causal effect of income inequality on health.
17.5.4.2.2 Regional and Cohort Level Data
Conditional on average regional income, life expectancy is sometimes negatively associated with regional income inequality. The negative relationship holds across US states but not at lower levels of aggregation (metropolitan areas, cities)58 and the evidence is
There is a significant US county level association between income inequality and mortality (Yang et al., 2012).
mixed in other countries (Deaton, 2003; Leigh et al., 2009; Lynch et al., 2004a; Subramanian and Kawachi, 2004; Wagstaff and van Doorslaer, 2000; Wilkinson and Pickett, 2006). The state-level association in the USA could either indicate a causal mechanism or greater aggregation bias at that level. Inclusion of state-level variables eliminates (or dramatically reduces) the association, although these may be mediators rather than confounders (Subramanian and Kawachi, 2004; Wilkinson and Pickett, 2006). The racial composition of US states, a control that knocks out the effect of income inequality, might itself be related to the provision and quality of publicly provided health care (Ash and Robinson, 2009; Deaton and Lubotsky, 2009) (Table 17.9). That statelevel income inequality loses much of its explanatory power for mortality after conditioning on measures of social cohesion and interpersonal trust has been interpreted as indicative of a mechanism operating through social capital (Kawachi et al., 1997). Missing from this argument is evidence of a causal effect of income inequality on social capital.
USA and UK birth cohort studies find no association between mortality and income inequality (Deaton and Paxson, 2001, 2004).
17.5.4.2.3 Individual-Level Data
There is little support for an association between individual mortality and income inequality conditional on individual income. This holds both in studies exploiting regional variation in income inequality, which risk confounding from regional health effects, and in studies exploiting within-country time variation in income inequality, which risk confounding from time trends (Deaton, 2003; Lynch et al., 2004a,b; Subramanian and Kawachi, 2004; Wagstaff and van Doorslaer, 2000). Morbidity measures, which are more commonly available at the individual level, also have no association with income inequality outside the USA. There is evidence that income inequality at the state level, but again not lower levels, is negatively correlated with the physical and mental health of the poorest individuals in the USA. But this could simply result from state-level income inequality picking up the effect of state-level differences in public policies toward the poor (Mellor and Milyo, 2002) (Table 17.10).
Analyses of individual-level (pseudo) panel data find no association between mortality or morbidity and income inequality. Using high-quality Swedish administrative data with more than 10 years of follow up on income and vital status, Gerdtham and Johannesson (2004) find no effect of municipality-level income inequality on mortality after conditioning on individual income and average municipality income. There is also no relationship of income inequality with SAH revealed by analyses of 12 years of British panel data allowing for unobserved heterogeneity (Lorgelly and Lindley, 2008) and 22 years of British repeated cross-section data (Gravelle and Sutton, 2009). Neither is mental health correlated with income inequality in Australian panel data (Bechtel et al., 2012).
Cross-country studies of individual-level data largely corroborate the negative finding. There are statistically significant, but economically negligible, effects of regional and nationwide income inequality on SAH in panel data on 11 European countries between 1994 and 2001 (Hildebrand and Kerm, 2009). Combining micro data from Australia, Germany, the UK, and the USA with country-level tax records on the income share of the richest percentile (Atkinson et al., 2011), Lillard et al. (2012) find that a higher- income share of the rich is associated with worse SAH, but once time trends are accounted for, the pattern reverses or disappears. The authors also find no evidence that income inequality during the first 20 years of life impacts on current SAH.
Pooling cross-section data for 21 countries, and subject to imposing the same relationship between health and individual income across all those countries, Karlsson et al. (2010) find that health is negatively correlated with income inequality in high-income countries, but there is no relationship in middle- and low-income countries. However, with point-in-time cross-country variation, one can never be sure that the income inequality effect is distinguished from health variation across countries for any other reason. In China, SAH has been found to be positively associated with community-level income inequality at relatively low levels of inequality, but the association turns negative at higher inequality (Li and Zhu, 2006). Correcting for unobserved heterogeneity using panel data, the negative relationship persists and is stronger for poorer individuals (Fang and Rizzo, 2012). While consistent with the income inequality hypothesis, it is possible that this finding is driven by nonlinearity between income and health that is not fully captured in the specification adopted. Child undernutrition in a much lower-income country, Zambia, has been found to be negatively correlated with economic inequality (Nilsson and Bergh, 2013).
If there is health-related migration across regions with differing levels of inequality, perhaps because of differences in medical care, then estimates from the regression of individual health on regional inequality will be biased. One study avoids this by using the random assignment of refugees to a first area of residence in Sweden (Gronqvist et al., 2012). Despite the fact that the range of income inequality across years and municipalities is— perhaps surprisingly—of similar magnitude in Sweden, as it is in the USA or the UK, hospitalizations, sickness leave and mortality were all found to be unrelated to municipality income inequality. Because refugees are likely to be much poorer and to have quite different references from the general population, one may doubt whether this analysis reveals much about either the income inequality or relative hypotheses that can be generalized.
Finally, some studies find that higher levels of social capital are associated with better individual health (Petrou and Kupek, 2008; van Groezen et al., 2011), and others confirm this when using instruments to deal with potential endogeneity of measures of social capital (d’Hombres et al., 2010; Ronconi et al., 2012). None of these studies test whether social capital itself responds to income inequality.
17.5.4.3 Relative Hypotheses
The only study that seeks to test all the relative hypotheses (income, deprivation, and position) rejects all three in favor of the absolute income hypothesis as an explanation of variation in SAH, using UK longitudinal data (Lorgelly and Lindley, 2008). Inconsistent with the relative income hypothesis, conditional on individual income, mortality is found to be lower among individuals living in Swedish municipalities with higher average incomes (Gerdtham and Johannesson, 2004). In contrast, mortality risk, especially for black males, is positively correlated with community average income in the USA (Miller and Paxson, 2006). Data on SAH from 11 European countries are consistent with the relative income hypothesis for males, although the negative correlation of health with average regional income is very small in magnitude, but, if anything, women report slightly better health when regional income is higher (Hildebrand and Kerm, 2009). There is little evidence in favor of the relative income hypothesis in the UK data on SAH (Gravelle and Sutton, 2009).
Analyses of data from Australia (Bechtel et al., 2012), China (Li and Zhu, 2006), and the UK (Gravelle and Sutton, 2009; Jones and Wildman, 2008) find little or no evidence consistent with the relative deprivation hypothesis.[109] Although one of the UK studies finds that mental health does fall slightly with relative deprivation ( Jones and Wildman, 2008), which is consistent with other evidence that mental health, but not physical health or longevity, is negatively associated with relative deprivation (Adjaye-Gbewonyo and Kawachi, 2012). One analysis of the US data on mortality and SAH does find evidence consistent with the relative deprivation hypothesis when reference groups are defined narrowly (based on race, state, education, and age) rather than more broadly (state only), as is the case with most other studies (Eibner and Evans, 2005).
17.5.5 Conclusion
The claim that income inequality is harmful to health has provoked much empirical research. This research has delivered little credible evidence to support the hypothesis that income inequality negatively impacts the health of all individuals in society, however. Average population health is negatively associated with income inequality across high- and middle-income countries, but there is no association through time or across regions within countries, except in the USA where state-level differences in health seem to be related to racial composition and possibly also social capital. Individual-level data on morbidity and mortality from high-income countries display no significant, nonne- gligible relationship to income inequality after controlling for individual income. Few studies have designs capable of testing the hypotheses that relative income, deprivation, or economic position causally impact health. The evidence that exists shows little support for these hypotheses, except maybe for a negative impact of relative deprivation on mental health. But research has yet to fully separate relative from absolute income effects, investigate the strong possibility that health determines relative economic status, and create an appropriate definition, and thus potential endogeneity, for reference 60
59
groups.
The lack of evidence might reflect a lack of well-defined theory and, consequently, precision in the way in which empirical analyses relate to hypotheses. Several potential mechanisms, including public provision of goods, social capital, psychosocial mechanisms, and pecuniary externalities, have been proposed, but all lack a precise description of how income inequality and/or relative income impact health. The distinction between the hypotheses is not clear; the relative hypotheses are often claimed to imply an effect of income inequality on the health of all individuals, and it is not clear whether the three relative hypotheses are intended to derive from distinct mechanisms. Psychosocial effects are often loosely cited as the main potential mechanism without specification of how, and for whom, relative economic status provokes stress. Further, it is not clear why priority should be given to relative income, as opposed to some other dimension of socioeconomic position, as a cause of psychosocial stress.
A cheap call for research designs capable of identifying the impact of income inequality on health would be unhelpful. Sound identification of a causal effect of income on health is difficult enough. Obtaining exogenous variation in income inequality is an even more daunting task. Rather than further searching for a significant effect of income inequality on health, a more fruitful research agenda would be to directly investigate the causal mechanisms through which health may be related to income inequality. For example, studies have shown that individual health and social capital are associated, but whether this is the result of causality has not received sufficient attention.
17.6.
More on the topic ECONOMIC INEQUALITY AS A DETERMINANT OF HEALTH:
- Contents
- CONTENTS
- INTRODUCTION
- INEQUALITY OF OPPORTUNITY: MEASUREMENT ISSUES AND EMPIRICAL RESULTS
- THE ROLE OF POLICY
- INTRODUCTION
- PREVIOUS LITERATURE
- EMPIRICAL FINDINGS
- THE POSITIVE ECONOMICS OF INCOME DISTRIBUTION
- Concluding remarks