35 Infertility and Assisted Reproductive Technologies
Cindy M. P. Duke
Mindy S. Christianson
INFERTILITY
Definitions
• Infertility: failure of a couple of reproductive age to conceive after at least 1 year of regular coitus without contraception
• Primary infertility: infertility in a woman who has never been pregnant
• Secondary infertility: infertility in a woman who has had one or more previous pregnancies
• Fecundability: probability of achieving pregnancy within one menstrual cycle.
For a normal couple, this is approximately 25%.• Fecundity: ability to achieve a live birth within one menstrual cycle
Incidence
• Data from the 2002 National Survey of Family Growth (NSFG) revealed that 2% of women of reproductive age in the United States had an infertility-related medical appointment within the past year.
• Data from the 2006 to 2010 NSFG continued to show that as in the 2002 data, 11.9% of women of reproductive age reported having received infertility services at some point in their lives.
• Additionally, 6% of couples with women of reproductive age reported not becoming pregnant after not using contraception in the prior year.
P.468
TABLE 35-1 Differential Diagnosis of Infertility
| Diagnosis | Percent | Basic Evaluation |
| Male factors | 30 | Semen analysis |
| T ubal/uterine/peritoneal factors | 25 | HSG, laparoscopy, chromopertubation |
| Anovulation/ovarian factors | 25 | BBT chart, midluteal progesterone level, endometrial biopsy, luteinizing hormone testing |
| Cervical factors | 10 | Postcoital test |
| Unexplained infertility | 10 | All of the above |
HSG, hysterosalpingogram; BBT, basal body temperature.
Adapted from Fritz MA. Infertility. In Fritz MA, Speroff L, eds. Clinical Gynecologic Endocrinology and Infertility, 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010:1137-1190.• Demand for infertility services has increased in recent years. Reasons include the following:
• Delayed childbearing in women due to career demands and marriage at a later age
• An increase in variety and effectiveness of assisted reproductive technology (ART) treatments and an increased public awareness of these treatments, including in vitro fertilization (IVF)
• An increase in tubal factor infertility as a consequence of sexually transmitted diseases
• Relative scarcity of babies placed for adoption due to effective contraception and increased availability of abortion services.
Differential Diagnosis
• The differential diagnosis of infertility encompasses five principal categories (Table 35-1):
• Male factor
• Ovulatory dysfunction
• Structural (tubal/peritoneal and uterine)
• Cervical factors
• Unexplained causes
• Coital factors
EVALUATION
• Evaluation is indicated for women who fail to conceive after 1 or more years of regular, unprotected intercourse.
• Women older than the age of 35 years should be evaluated sooner (i.e., after 6 months of regular, unprotected intercourse).
• Successful reproduction requires proper structure and function of the entire reproductive axis, including hypothalamus, pituitary gland, ovaries, fallopian tube, uterus, cervix, and vagina.
• Infertility evaluation comprises six major elements:
• History and physical examination
• Semen analysis
P.469
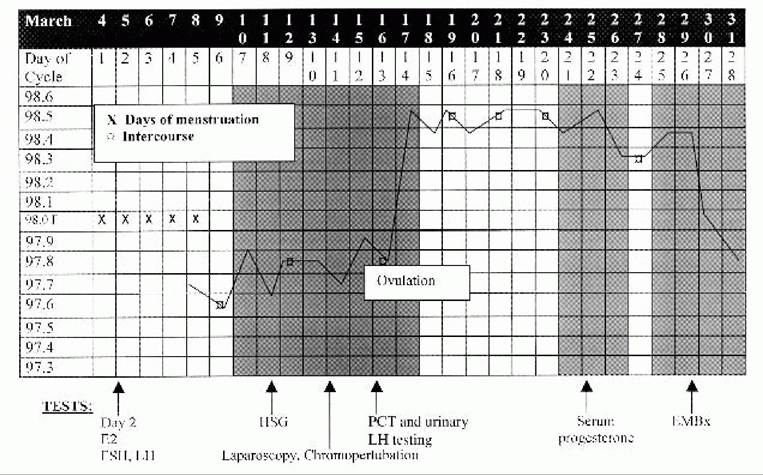
Figure 35-1. Sample basal body temperature (BBT) chart with complete infertility evaluation within one menstrual cycle. E2, estradiol level; EMBx, endometrial biopsy; FSH, folliclestimulating hormone level; LH, luteinizing hormone level; HSG, hysterosalpingogram; PCT, postcoital test.
• Assessment of ovarian reserve
• T ests for occurrence of ovulation
î Tests to evaluate for structural abnormalities: These include evaluation of tubal patency, detection of uterine abnormalities, and determination of peritoneal abnormalities.
• Sperm—cervical mucus interaction (postcoital testing [PCT])—for select patients. This has fallen out of favor and is infrequently used.
• With proper coordination, the evaluation can be completed within one menstrual cycle (Fig. 35-1). No abnormality or cause of infertility is identified in 10% to 15% of couples. This group comprises a category known as “unexplained infertility.”
History and Physical Examination
• The initial assessment involves an extended and complete history from both partners and a complete physical examination.
• Physical examination of the male partner can be deferred pending the results of the semen analysis. Abnormal results of a semen analysis warrants referral to a urologist.
• History elicited from both male and female partners should include the following:
• Duration of infertility, methods of contraception, previous evaluation and treatment, prior reproductive history, sexual dysfunction, coital frequency and satisfaction, sexually transmitted infections, tobacco and alcohol use, caffeine use, family history of mental retardation, and birth defects
• History elicited from the female partner should include the following:
• Complete menstrual history, dysmenorrhea or menorrhagia, pelvic or abdominal pain, dyspareunia, symptoms of thyroid disease, galactorrhea, symptoms of hirsutism, exercise habits, and indices of stress
P.470
• Components of the female physical exam should include the following:
• Weight and body mass index, thyroid exam, breast exam, signs of hirsutism, pelvic or abdominal tenderness, uterine size and mobility, adnexal masses and/or tenderness, cul-de-sac tenderness, or nodularity
• Baseline studies and labs may include the following: thyroid-stimulating hormone, prolactin, folliclestimulating hormone (FSH), 17-hydroxyprogesterone, serum testosterone, progesterone, dehydroepiandrosterone (DHEAS), semen analysis, and hysterosalpingogram (HSG).
Male Factor Infertility Evaluation
• The semen analysis is the cornerstone of male factor infertility evaluation.
• Semen sample should be collected after at least 48 to 72 hours abstinence and is best evaluated within 1 hour of ejaculation.
• Obtained either by masturbation or by sexual intercourse with a silicone condom because latex condoms are spermicidal.
• Lower reference limits (normal parameters) according to the World Health Organization (WHO) are as follows:
• Ejaculate volume of at least 1.5 mL
• Semen pH above 7.2
• Sperm concentration of at least 20 million/mL
• Greater than 40% total motility; greater than 32% progressive motility
• Greater than 4% normal morphology
• Semen analysis terminology:
• Azoospermia: absence of sperm in the ejaculate
• Oligospermia: a concentration of fewer than 20 million sperm/mL
• Asthenospermia: reduced sperm motility
• Men with an abnormal semen analysis should be referred to a urologist, especially in cases of oligospermia or azoospermia. Causes of male factor infertility include the following:
• Klinefelter syndrome
î Karyotype is 47, XXY.
î Most common genetic anomaly in azoospermic men
î Found in 1:500 to 1:1,000 live male births
î Incidence: 3% of infertile men, 3.5% to 14.5% of azoospermic men, 1 % of couples referred to intracytoplasmic sperm injection (ICSI)
• Congenital absence of the vas deferens (CAVD)
î Associated with cystic fibrosis gene mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
î Partners of men with CAVD must be tested for the CFTR gene mutation before pursuing infertility treatment with retrieved sperm.
• Y-chromosome microdeletions
î May be found in up to 7% of men with male factor infertility
î Although these men may be able to father children via IVF/ICSI, male offspring will inherit the Y- chromosome microdeletion and be infertile.
Exclusion of ovulatory factor infertility
To exclude ovulatory dysfunction, the presence of ovulation must be confirmed.
In addition, ovarian reserve should be assessed to exclude oocyte depletion and premature ovarian failure.P.471
Confirmation of Ovulation
• The basal body temperature (BBT) chart (see Fig. 35-1) is a simple means of determining whether ovulation has occurred.
• The woman's temperature is taken daily on awakening, before any activity, and recorded on a graph.
• After ovulation, rising progesterone levels increase the basal temperature by approximately 0.4°F (0.22°C) through a hypothalamic thermogenic effect.
• Because the rise in progesterone may occur anytime from 2 days before ovulation to 1 day after, the temperature elevation does not predict the exact moment of ovulation but offers retrospective confirmation of its occurrence.
• A temperature elevation is usually sustained for 14 ± 2 days. One that persists for 3.0 ng/mL in a blood sample drawn between days 19 and 23 suggests ovulation has occurred. Normal adequate luteal support usually produces a progesterone concentration >10 ng/mL.
• Daily monitoring of urinary luteinizing hormone (LH) is now widely used, given the proliferation of commercial tests for home use.
• Using a threshold concentration of 40 mIU/mL, positive testing for urinary LH correlates well with the surge of serum LH levels that trigger ovulation.
Assessment of Ovarian Reserve
• Depleted ovarian reserve adversely impacts fecundability given the inferior quantity and quality of remaining oocytes. The following tests help identify both a depleted reserve and the likelihood of response to controlled ovarian hyperstimulation (COH) during assisted reproduction:
• Day 3 FSH concentration: Values below 10 to 15 mIU/mL suggest adequate ovarian reserve. The exact cutoff depends on the particular laboratory reference standards.
• Measurement of anti-mullerian hormone (AMH) levels can also be helpful in predicting ovarian reserve. AMH is a measure of the primordial follicle pool and over a woman's reproductive lifetime steadily decreases to undetectable levels by menopause.
There are kits available to assay for this hormone and the exact cutoff depends on the specific laboratory/assay reference standard.• Imaging of antral follicle counts by ultrasonography
• Clomiphene citrate challenge test: The administration of clomiphene citrate 100 mg orally on menstrual cycle days 5 to 9 with measurement of day 3 and day 10 FSH. An exaggerated FSH response portends poorly for spontaneous or assisted conception.
EXCLUSION OF STRUCTURAL FACTORS (TUBAL/PERITONEAL AND UTERINE)
• Tubal/peritoneal factors include endometriosis, pelvic adhesion disease, or previous bilateral tubal ligation. Uterine factors include leiomyomata, intrauterine synechiae (Asherman syndrome), septae, and other mullerian anomalies.
• HSG assesses uterine and fallopian tube contour and tubal patency (Fig. 35-2).
• HSG shows appreciable mullerian anomalies as well as most endometrial polyps, synechiae, and submucosal fibroids. It can also determine tubal patency.
• Performed in the early follicular phase, within 1 week of cessation of menstrual flow, to minimize chances of interrupting a pregnancy
P.472
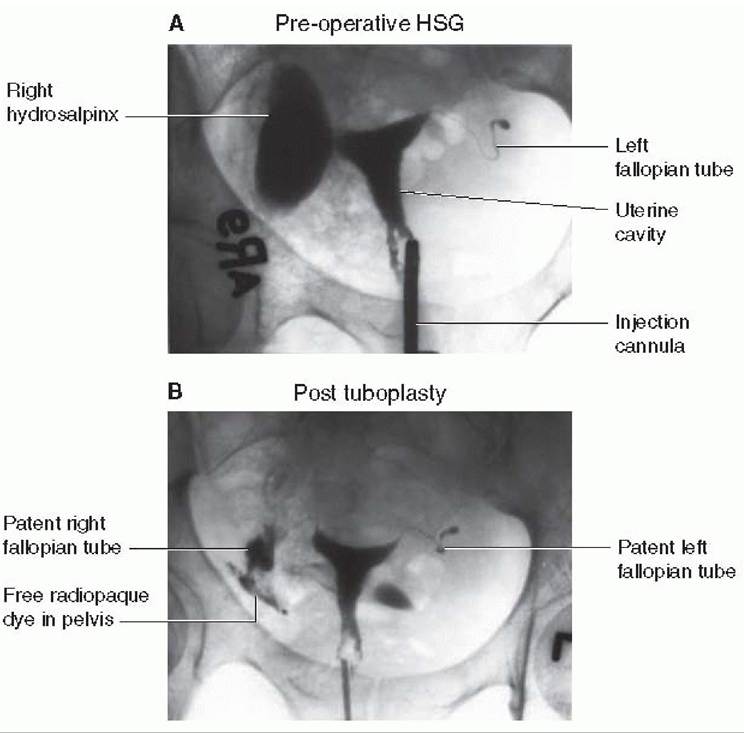
Figure 35-2. Hysterosalpingogram showing large right hydrosalpinx (A) that is resolved following successful tuboplasty (B). Real-time radiographs are obtained as radiopaque dye is injected through a cannula inserted in the cervical canal. Normal patent tubes demonstrate bilateral spillage from the fallopian tubes into the pelvis. (Original images courtesy of Dr. Edward Wallach, Johns Hopkins Hospital,
Department of Gynecology and Obstetrics, Division of Reproductive Endocrinology and Infertility.)
• The procedure is performed by injecting a radiopaque dye through the cervix. As more dye is injected, the dye normally passes through the uterine cavity into the fallopian tubes and then spills into the peritoneal cavity.
• X-ray films are taken under fluoroscopy to evaluate tubal patency.
• Nonsteroidal anti-inflammatory drugs may be given to prevent cramping.
• HSG may have therapeutic effects. Several studies have indicated increased pregnancy rates for several months after the procedure.
• Prophylactic antibiotics (doxycycline, 100 mg orally twice daily for 5 to 7 days) are advisable when the patient has a history of pelvic inflammatory disease or when hydrosalpinges are identified during the study.
• Saline infusion ultrasonography (sonohysterography [SHG])
• SHG involves transvaginal ultrasound after the introduction of sterile water or saline into the uterine cavity.
P.473
• Useful in assessment of uterine cavity abnormalities such as polyps or submucosal fibroids
• Hysteroscopy
• Definitive method to evaluate the uterine cavity
• Reserved for those patients with HSG or SHG results that merit further evaluation. It offers the possibility of minimally invasive treatment at time of the procedure
• Diagnostic laparoscopy
• Assesses peritoneal and tubal factors, such as endometriosis and pelvic adhesions and can provide access for simultaneous corrective surgery
• Laparoscopy should be scheduled in the follicular phase. This is the final and most invasive step in the patient's evaluation.
• Findings on HSG correlate with laparoscopic findings 60% to 70% of the time.
• Chromopertubation: dye (usually a dilute solution of indigo carmine) instilled through the fallopian tubes during laparoscopy to visually document tubal patency
• Hysteroscopy may also be included to ensure that no intrauterine abnormalities were missed on the HSG.
EXCLUSION OF CERVICAL FACTOR INFERTILITY
• The PCT or Huhner test allows direct analysis of sperm and cervical mucus interaction and provides a rough estimate of sperm quality.
• The test is done between days 12 and 14 of a 28- to 30-day menstrual cycle (after 48 hours of abstinence) when maximum estrogen secretion is present and the mucus is examined within 2 to 12 hours.
• Because interpretation of the PCT is subjective, the validity of the test is controversial, despite its long history of use.
• The test's use is most valuable for patients with history or physical exam findings suggestive of cervical factor, when the results will help direct treatment. However, a finding of 5 to 10 progressively motile spermatozoa per high-power field and clear acellular mucus with a spinnbarkeit (the degree to which the mucus stretches
between two slides) of 8 cm generally suggests normal cervical function.
• Fecundity rates do not correlate directly with the number of motile sperm seen. The most common cause of an abnormal PCT is poor timing. Other causes include cervical stenosis, hypoplastic endocervical canal, coital dysfunction, and male factors. The sample can also be assessed for pH, mucus cellularity, white blood cell, and ferning. Clumping and flagellation of sperm without progression are often suggestive of antisperm antibodies.
ENDOMETRIAL BIOPSY AND THE LUTEAL PHASE DEFECT
• Endometrial biopsy, historically, can document ovulation by histologic demonstration of decidualized stroma, assess for endometritis, and allows for histologic dating of the endometrium within 2 to 3 days and usually performed between days 24 and 26 of a 28-day menstrual cycle or 2 to 4 days before anticipated menstruation.
• Dates of the biopsy and subsequent menstrual cycle have been used to determine whether a luteal phase deficiency—insufficient progesterone support for the purported histologic date of the endometrium—is present. However, recent reports have
P.474 demonstrated that fertile women were at least as likely as their infertile counterparts to have an out-of-phase endometrial biopsy suggestive of a luteal phase defect.
• At present, this approach is rarely used.
TREATMENT FOR INFERTILITY
Anovulation
The vast majority of anovulatory women of reproductive age fall into WHO class II and, fortunately, this class proves responsive to ovulation induction. The agents most commonly used to stimulate multiple ovarian follicles are clomiphene citrate, human menopausal gonadotropins (hMG), and purified FSH. The WHO stratifies anovulatory women into three classes:
• WHO class I: hypogonadotropic hypogonadal anovulation
• Hypothalamic amenorrhea attributable to low gonadotropin-releasing hormone (GnRH) levels or pituitary unresponsiveness to hypothalamic GnRH, with resultant low FSH and serum estradiol levels
• Causes include excessive weight gain or loss and exercise or emotional stress.
• WHO class II: normogonadotropic normoestrogenic anovulation
• Normal levels of estradiol and FSH; LH levels, however, are elevated. This class includes the polycystic ovarian syndrome (PCOS).
• WHO class III: hypergonadotropic hypoestrogenic anovulation
• Main causes include premature ovarian failure (no follicles due to early menopause) or ovarian resistance.
• These patients rarely respond to treatment for anovulation.
• Donor eggs may be best option for these patients in achieving pregnancy.
Clomiphene Citrate
• Mechanism of action: synthetic, nonsteroidal estrogen agonist-antagonist that increases the release of GnRH and subsequent LH and FSH release (antiestrogenic effect in hypothalamus results in increased GnRH secretion)
• Useful in women with oligomenorrhea and amenorrhea, with intact hypothalamicpituitary-ovarian axes
• Patients who are overweight and hyperandrogenic or hypoestrogenic have decreased responsiveness to CC.
• Initiated on day 3, 4, or 5 in the menstrual cycle, usually at a starting dose of 50 mg for 5 days
• Adverse effects: vasomotor symptoms such as headache and mood change; rarely, visual symptoms such as transient blurry vision or scotomata have been reported
• Complications: cystic ovarian enlargement and multifetal gestations (5% to 10% of pregnancies)
• Another option for ovulation induction particularly in anovulatory women (e.g., PCOS) is use of aromatase inhibitors.
• Current formulations involved are third-generation drugs letrozole (Femara) and anastrazole.
î In particular, letrozole has been shown to be effective in PCOS women who have failed CC induction.
î Letrozole is quickly absorbed via the gastrointestinal tract and metabolized and is generally considered safe for use.
• However, this use of aromatase inhibitors is off-label and based on limited data from one small study, patients must be counseled regarding possible risk of congenital anomalies, specifically possible risk of cardiac and bone malformations.
P.475
• This should also be tempered by the coexisting data from another small randomized trial looking at pregnancy outcomes following treatment with letrozole, anastrazole, or CC for induction which showed no increase in congenital anomalies.
Exogenous Gonadotropins
• GnRH, hMG, and FSH are used primarily in women who fail to respond to CC or who have hypogonadotropic amenorrhea or unexplained infertility.
• Prescription of these expensive drugs, which are used in the more complicated protocols for IVF (see the following text), should be left to specialists trained in their use.
Hyperprolactinemia
• Bromocriptine is used to induce ovulation in patients with hyperprolactinemia.
• Bromocriptine is a dopamine agonist that directly inhibits pituitary secretion of prolactin, which restores normal gonadotropin release.
• The usual starting dose is 2.5 mg at bedtime to prevent dopaminergic side effects, which include nausea, diarrhea, dizziness, and headache.
• If oral administration cannot be tolerated, vaginal administration is recommended.
• A response is usually seen in 2 to 3 months, and 80% of hyperprolactinemic patients ovulate and become pregnant.
• Cabergoline is an alternative for those who do not tolerate bromocriptine.
Thyroid Dysfunction
• Both hypothyroidism and hyperthyroidism can lead to anovulation with subsequent infertility. These medical conditions should be corrected prior to a patient attempting pregnancy. See Chapter 13.
Hypothalamic-Pituitary Axis Dysfunction
• Hypothalamic-pituitary axis problems including extreme weight gain or loss, excessive exercise, and emotional stress can all impact the secretion of GnRH from the hypothalamus and cause ovulatory dysfunction. These must be addressed by appropriate behavioral or psychological intervention.
Male Factor Infertility
• Although the gynecologist does not directly treat male patients, therapies to treat male factor infertility often involve hormonal manipulation in the female partner. The evaluation is analogous to that in the woman, with examination of the hypothalamic-pituitary-testicular axis, outflow tract, and testicular function.
• Toxins, viruses, sexually transmitted diseases, varicoceles, and congenital problems can all influence infertility.
• The procedure of ICSI has revolutionized treatment of male infertility. As long as viable sperm can be retrieved by ejaculation, epididymal aspiration, or testicular biopsy, successful fertilization and pregnancy can be achieved. The fertilization rate is 95%, and the pregnancy rate is comparable to that of IVF.
Endometriosis
• Endometriosis is the ectopic growth of hormonally responsive endometrial tissue and accounts for 15% of female infertility. Surgical treatment may be effective, although management by an infertility specialist for IVF may be necessary. See Chapter 38.
P.476
Luteal Phase Defects
• Luteal phase defects are thought to occur in both fertile and infertile women, and the role for treatment is highly controversial. Nevertheless, in a couple with documented infertility, it is not unreasonable to treat a presumed luteal phase deficiency with intramuscular or intravaginal progesterone in the postovulatory phase of the cycle and, if pregnancy occurs, until the luteoplacental shift occurs.
Uterine Factors
• Uterine factors, such as submucous leiomyomas, intrauterine synechiae (Asherman syndrome), and uterine deformities such as septa, cause approximately 2% of infertility. The mainstay of treatment for these conditions is surgical correction, frequently via a hysteroscopic approach.
Infections
• Infections of the female and male genital tracts have been implicated as causes of infertility. Chlamydia infection and gonorrhea are the major pathogens and should be treated appropriately. Ureaplasma urealyticum and Mycoplasma hominis have also been implicated, and, if positively identified by culture, they should be treated with oral doxycycline, 100 mg twice daily for 7 days. This has been shown to increase the pregnancy rate in patients with primary infertility.
Tubal Factor Infertility
• Tubal factor infertility has become more prevalent with the increased incidence of salpingitis. The frequency of tubal occlusion after one, two, and three episodes of salpingitis is reported to be 11 %, 23%, and 54%, respectively. Appendicitis, previous abdominopelvic surgery, endometriosis, and ectopic pregnancy can also lead to adhesion formation and damaged tubes.
• Proximal tubal obstruction is identified on HSG. Tubal spasm may mimic proximal obstruction, however, and obstruction should be confirmed by laparoscopy. Treatment consists of tubal cannulation, microsurgical tubocornual reanastomosis, or IVF.
• Distal tubal disease or distortion can be seen on HSG and laparoscopy. The success of corrective surgery (neosalpingostomy) depends on the extent of disease.
• If IVF is pursued in patients with tubal factor infertility, several studies have shown that success rates of IVF are improved if hydrosalpinges are removed.
• For patients with a history of a prior bilateral tubal ligation who desire fertility, options include microsurgical sterilization reversal as well as IVF.
• Success of tubal reanastomosis depends on age, type, and location of the sterilization procedure and final lengths of repaired fallopian tubes.
• IVF may be a better option for patients who desire only a single additional child.
ASSISTED REPRODUCTIVE TECHNOLOGIES
• Since the first successful IVF pregnancy delivered in 1978, several techniques have been developed that enhance our ability to overcome infertility.
• Among them are the capabilities for embryo cryopreservation and ovum donation.
• Of all ART cycles nationwide using fresh nondonor eggs or embryos, 36.9% resulted in pregnancy according to the 2010 National Summary T ables and Fertility Clinic data, with 81.8% of these pregnancies resulting in a live birth of one or more infant.
P.477
• The majority (57.1%) of IVF pregnancies resulted in single live births, whereas 24.8% resulted in multipleinfant births. Miscarriages occurred in 16.1%, ectopic pregnancies in 0.7%, and stillbirths in 0.6%. The following types of procedures are currently used in ART.
Intrauterine Insemination
• May increase cycle fecundity when semen analysis contains decreased numbers of total motile sperm (absence of fimbria, severe adhesive disease, repeated ectopic pregnancies, or failed reconstructive therapy, also women with previous bilateral tubal ligation who chose IVF over reanastomosis
• Endometriosis: if other forms of treatment have failed
• Unexplained infertility
• Male factor infertility: low sperm count, low sperm motility, and abnormal morphology associated with reduction in fertilizing ability
• Uterine malformations: related to diethylstilbestrol exposure
• HIV-positive serodiscordant couples: Use of ICSI or sperm-washing techniques has enabled HIV-negative women to safely achieve pregnancy using the sperm of their affected male partners. Processing and handling of these specimens
P.479 require specialized facilities, protocols, training, and equipment to prevent cross contamination.
• Men and women seeking fertility preservation: patients about to undergo chemotherapy or irradiation of their pelvic regions can consider cryopreservation of gametes, embryos, or ovarian tissue for subsequent childbearing via ART.
• Couples seeking preimplantation genetic diagnosis (see later discussion).
CONTROLLED OVARIAN HYPERSTIMULATION AND PROTOCOLS FOR IN VITRO FERTILIZATION
The agents most commonly used to stimulate multiple ovarian follicles are CC, hMG, and purified FSH. The particular products and protocols used may be tailored as the treatment progresses to boost the chances of an adequate response and increase the pregnancy rate.
Clomiphene-Only Regimens
• These regimens are generally given on days 5 to 9 of the menstrual cycle.
• Response may be followed by BBT measurement, ultrasonography, and measurement of LH and estradiol levels.
• CC is inexpensive and has a low risk of ovarian hyperstimulation syndrome (OHSS). However, it creates a low oocyte yield (one or two per cycle), most commonly used with timed intercourse at home or IUI.
• Most treatment regimens start with 50 mg/day for 5 days beginning on cycle day 3 or day 5. If ovulation fails to occur, the dose may be increased to 100 mg/day.
• hCG, 5,000 IU to 10,000 IU, may be used to simulate an LH surge. Eighty percent of properly selected couples will conceive in the first three cycles after treatment. The most commonly used hCG formulation is choriogonadotropin alfa injection (Ovidrel).
• Potential side effects of CC are vasomotor flushes, blurring of vision, urticaria, pain, bloating, and multiple gestations (5% to 7% of cases, usually twins).
Gonadotropin Regimens
• These regimens increase the number of recruited follicles in patients who do not achieve pregnancy with CC and in those patients with endometriosis or unexplained infertility.
• hMG, which is a combination of LH and FSH, is usually given for 2 to 7 days.
• Although gonadotropin injections prove more effective at COH than clomiphene, they are more expensive and can lead to life-threatening OHSS.
• Trade names for hMG include Humegon, Pergonal, and Repronex.
• Attempts to minimize the potentially deleterious LH component of hMG have led to the manufacture of purified urinary FSH and, more recently, recombinant FSH.
• The purity and consistency associated with recombinant FSH argue for its exclusive use, but evidence of its superior efficacy has been conflicting and inconclusive. Follicle maturation during COH is monitored using sonography and serial measurement of estradiol levels.
• To complete oocyte maturation, hCG is administered once the follicles have reached 17 to 18 mm in diameter.
• Potential disadvantages of gonadotropin use include premature luteinization, spontaneous LH surges resulting in high cancellation rates, multiple gestations, and ovarian hyperstimulation.
P.480
Gonadotropin-Releasing Hormone Agonists
• These are used via a flare-up protocol or a luteal phase protocol in IVF cycles.
• The flare-up protocol causes an elevation of FSH in the first 4 days, which increases oocyte recruitment.
• After 5 days of administration, the GnRH agonist (GnRHa) downregulates the pituitary to prevent premature luteinization and a spontaneous LH surge.
• The luteal phase protocol involves starting GnRHa administration on the 17th to 21st menstrual day in the cycle before IVF.
• GnRHa increases the number, quality, and synchronization of the oocytes recovered per cycle and thereby improves the fertilization rate, the number of embryos, and the pregnancy rate.
• Lupron is the most commonly used GnRHa in the United States.
Gonadotropin-Releasing Hormone Antagonists
• Commonly used for COP in IVF cycles
• These block LH secretion, and the premature LH surges that force cycle cancellation without causing a flare- up effect.
• They are administered in a single dose on the eight menstrual day or in smaller doses over 4 days.
• Because they block the periovulatory LH surge, less gonadotropins are required to stimulate ovulation and side effects are decreased.
• Trade names include Antagon and Cetrotide.
OOCYTE RETRIEVAL, CULTURE FERTILIZATION, AND TRANSFER
There are two major techniques of oocyte retrieval. The most commonly used method is ultrasonographically guided follicular aspiration and the less common and rarely used method is laparoscopic oocyte retrieval.
Ultrasonographically Guided Oocyte Retrieval
• A 17-gauge needle passed through the vaginal fornix to retrieve oocytes.
• Performed 34 to 36 hours after hCG injection under sedation
• Potential complications include risk of bowel injury and injury to pelvic vessels.
Oocyte Fertilization
• Sperms are diluted, centrifuged, and incubated before 50,000 to 100,000 motile spermatozoa are added to each Petri dish containing an oocyte.
• Fertilization is documented by the presence of two pronuclei and extrusion of a second polar body at 24 hours.
Embryo T ransfer
• Performed 3 to 5 days after oocyte insemination
• Day 5 blastocyst transfer is becoming more common today due to higher livebirth rates compared to cleavage-stage (day 3) embryos.
• Excess embryos not used for transfer can be cryopreserved for an unlimited period, with a survival rate of 75%.
• The actual number of embryos transferred depends on the individual’s age and other risk factors for multiple pregnancy.
P.481
• The common practice is to supplement the luteal phase with progesterone given intramuscularly or by vaginal suppository, beginning the day of oocyte release and continuing into the 12th week of pregnancy.
MATERNAL, FETAL, AND LONG-TERM EFFECTS OF ASSISTED REPRODUCTIVE TECHNOLOGY
Ovarian Hyperstimulation Syndrome
• OHSS can be a life-threatening complication of COH characterized by ovarian enlargement and increased capillary permeability.
• Potentiated by COH cycles using GnRH analogs for downregulation or hCG to trigger oocyte maturation
• Presentation: abdominal bloating, ascites, decreased urine output, hemoconcentration, hypercoagulability,
hydrothorax, acute respiratory distress syndrome, electrolyte imbalance, and multiple organ failure
• Classified as mild, moderate, or severe according to the presenting symptoms
• Pathophysiology: thought to be mediated by vascular endothelial growth factor, produced by the ovary in response to LH or hCG
• Risk factors: young age, pregnancy, low body weight, high or rapidly climbing estradiol levels, large size and number of follicles, and the presence of PCOS
• T reatment: Moderate to severe cases of OHSS should be managed as an inpatient.
• Includes close monitoring of fluid and renal status, frequent evaluation of electrolytes and coagulation studies, intravascular resuscitation, thrombosis prophylaxis and paracentesis, and/or thoracentesis, as indicated
• Prevention: If impending OHSS is suspected, prevention can be attempted by lowering or withholding (“coasting”) the hCG triggering dose, postponing embryo transfer, or canceling the cycle.
• OHSS is an entirely iatrogenic entity that is usually avoidable by vigilance and judicious execution and alteration of COH regimen.
Multiple Gestation
• The 2010 data demonstrate that 30% of clinical pregnancies involved multiple gestation: 29.0% were twin pregnancies and 1% were triplet or higher order pregnancies.
• In attempting to limit the prevalence of multiple gestation, the American Society for Reproductive Medicine has issued practice recommendations governing the number of embryos transferred. These recommendations are stratified depending on whether cleavage-stage embryos or blastocysts are transferred.
• Women younger than age 35 years: strong consideration to transfer just one embryo if a favorable prognosis; no more than two embryos (cleavage stage or blastocyst) should be transferred
• Women aged 35 to 37 years: two cleavage-stage embryos if a favorable prognosis, otherwise three cleavage-stage embryos may be transferred; no more than two blastocysts may be transferred
• Women aged 38 to 40 years: three cleavage-stage embryos or two blastocysts if a favorable prognosis, otherwise four cleavage-stage embryos or three blastocysts may be transferred
• Women older than age 40 years: should receive no more than five cleavage-stage embryos or three blastocysts
• Should multiple gestation ensue, recourse to selective fetal reduction is available for patients who are comfortable with the ethics and risks of that procedure.
P.482
Heterotopic Pregnancy
• Occurs in up to 1 % of pregnancies after ART
• This incidence is dramatically higher than the corresponding ratio in the general population (1 in 30,000).
• The finding of an intrauterine pregnancy (IUP) in a woman who has undergone ART should not be automatically considered a reassuring finding, as the presence of a coexisting ectopic pregnancy is possible.
• Women, after ART who display signs or symptoms suggesting ectopic pregnancy must be closely followed despite confirmation of an IUP.
Effects of In Vitro Fertilization
• Inconsistent and equivocal evidence links IVF to increased risks of neonatal morbidity, birth defects, developmental disabilities, or certain childhood cancers.
• Conclusive evidence, however, does link IVF to an increased risk of low-birthweight deliveries even among full-term, singleton neonates. Most recent studies and data suggest that although fetuses resulting from ART are at higher risk of congenital abnormalities when compared to spontaneously conceived fetuses, the associated risk appears to be lower than previously believed and this is in part due to the recognition that some parental factors may play a role in this increased risk as opposed to simply the practice/inherent science of ART.
Effects of Intracytoplasmic Sperm Injection
• ICSI has been associated with a significant increase in sex and autosomal chromosome abnormalities and, potentially, with an increased risk of imprinting disorders, such as Beckwith-Wiedemann or Angelman syndromes.
• If a male with a Y chromosome microdeletion undergoes ICSI/IVF, male offspring will inherit the same microdeletion and, thus, also have male factor infertility.
NEW TECHNOLOGIES AND SOCIAL IMPLICATIONS
The advent of ART has raised unique ethical and social implications for couples undergoing such treatments. It has also presented an option for future childbearing with biologic offspring to individuals diagnosed with malignancies that require treatments with agents (chemotherapy, radiation, etc.) that can deplete ovarian or sperm reserve.
Embryo Cryopreservation
• It is now common practice to cryopreserve excess embryos not used during an embryo transfer cycle.
• Although many couples will use these embryos for future cycles, the number of cryopreserved embryos in the United States is estimated to be over 400,000.
• Disposition options for supernumerary cryopreserved embryos include use, discard, donation to research (including stem cell research), donation to other couples, future embryo transfer, or continued storage.
• It is imperative that couples be aware that excess embryos could result from ART and that a plan be discussed in advance for these embryos.
Oocyte Cryopreservation and Ovarian Tissue Preservation
• The development of more reliable and reproducible freezing and thawing protocols, namely vitrification, has resulted in egg (oocyte) cryopreservation becoming widely available and no longer considered experimental.
P.483
• Oocyte cryopreservation may be offered to any reproductive age woman who is about to undergo/initiate treatment with known gonadotoxic agents (e.g., chemotherapy) who has adequate time (2 to 3 weeks) to delay therapy for an IVF cycle.
• Oocyte freezing may also be offered to couples whose religious or ethical beliefs conflict with embryo cryopreservation or for women who plan to delay childbearing for nonmedical reasons.
• Ovarian tissue cryopreservation is a fertility preservation option for women without adequate time to freeze embryos or oocytes of prepubertal girls. It is considered highly experimental.
Third-Party Reproduction
• Includes donor oocytes and sperm, donated embryos, and gestational carriers (surrogates)
• Ethical issues involved include the following:
• Disclosure to children conceived by these technologies regarding their genetic origin
• Privacy issues for donors
• Compensation for oocyte donors and gestational carriers
Preimplantation Genetic Testing
• Umbrella term describing all types of genetic testing of the embryo. It is further subdivided into preimplantation genetic diagnosis (PGD) and preimplantation genetic screening (PGS).
• PGD allows couples with various single-gene disorders and X-linked genetic diseases to avoid transmission of the disorder to their offspring.
• PGD proceeds by biopsy and genetic analysis of one of the following specimens:
• One to two blastomeres of a cleavage-stage (days 2 to 3) embryo derived from IVF
• Polar body biopsy from a metaphase II oocyte obtained after COH
• T rophectoderm tissue from a blastocyst-stage (day 5) embryo
• Single-gene disorders
• Using polymerase chain reaction (PCR), DNA extracted from the biopsy specimen is used to screen for a known hereditary disorder—for example, cystic fibrosis, muscular dystrophy, hemophilia, or Huntington disease.
• Only unaffected preimplantation embryos would be transferred to the woman's uterus.
• Sibling human leukocyte antigen (HLA) matching
• PGD was first used in 2000 to screen for Fanconi anemia and simultaneously to select for a preimplantation embryo that was HLA matched to a preexisting sibling afflicted with this disorder.
• Aneuploidy testing
• Fluorescence in situ hybridization (FISH) is a molecular technique that uses chromosome-specific sequences that can be hybridized to complementary probes attached to differentially colored fluorochromes.
• FISH has been used for the PGD of aneuploidy and chromosomal abnormalities, such as translocations.
• One drawback to FISH is that it only samples some of the chromosomes (no more than 14) but not all 23. Additionally, in the event of mosaicism, selective cell sampling—further compounded by selective chromosome screening—can lead to misdiagnoses.
P.484
• PGS is a screening test for aneuploidy (numerical chromosomal abnormalities) in embryos from parents that have no known chromosomal abnormality (normal karyotype).
• Methods to perform PGS include FISH, single nucleotide polymorphism (SNP) microarrays, and comparative genomic hybridization.
• A role for PGS is emerging in embryo screening in women of advanced maternal age, repeated miscarriage, and repeated otherwise unexplained IVF failure.
• PGS can screen for all 23 chromosomes and can help identify optimal (euploid) embryos for transfer before IVF. However, more data is needed to determine its effectiveness in predicting the ultimate genetic status of the fetus.
• Elective sex selection
• Also referred to as family balancing
• PGD, via either PCR or FISH, enables efficient and accurate gender selection by screening selectively for the Y chromosome.
• Sharp debate over the propriety of such nonmedical use of reproductive technology has limited the prevalence of this application.
SUGGESTED READINGS
Brezina P, Brezina DS, Kearns WG. Preimplantation genetic testing. BMJ 2012;345:e5908.
Centers for Disease Control and Prevention, National Center for Health Statistics. 2002 National Survey of Family Growth. U.S. Department of Health and Human Services Web site. http://www.cdc.gov/nchs/nsfg.htm. Accessed May 20, 2013.
Centers for Disease Control and Prevention, National Center for Health Statistics. 2006-2010 National Survey of Family Growth. U.S. Department of Health and Human Services Web site. http://www.cdc.gov/nchs/nsfg/abc_list_i.htmtfinfertility. Accessed May 20, 2013.
Centers for Disease Control and Prevention, National Center for Health Statistics. 2010 Assisted Reproductive Technology Report. U.S. Department of Health and Human Services Web site. http://www.cdc.gov/art/ART2010/index.htm. Accessed May 20, 2013.
Cooper TG, Noonan E, von Eckardstein S, et al. World Health Organization reference values for human semen characteristics. Hum Reprod Update 2010;16(3):231-245.
Davies MJ, Moore VM, Wilson KJ, et al. Reproductive technologies and the risk of birth defects. N Engl J Med 2012;366:1803-1813.
Glujovsky D, Blake D, Farquhar C, et al. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Syst Rev2012;(7):CD002118.
Hansen M, Kurinczuk JJ, Milne E, et al. Assisted reproductive technology and birth defects: a systematic review and metaanalysis. Hum Reprod Update 2013;19(4):330-353.
Legro RS, Barnhart HX, Schlaff WD, et al; Cooperative Multicenter Reproductive Medicine Network. Clomiphene, metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med 2007;356(6):551-566.
Practice Committee of the American Society for Reproductive Medicine. Preimplantation genetic diagnosis: a practice committee opinion. Fertil Steril 2008;90:S136-S140.
Practice Committee of the American Society for Reproductive Medicine; Practice Committee of the Society for Assisted Reproductive Technology. Criteria for number of embryos to transfer: a committee opinion. Fertil Steril 2013;99(1):44-46.
Practice Committee of the American Society for Reproductive Medicine; Practice Committee of the Society for Assisted Reproductive Technology. Mature oocyte cryopreservation: a guideline. Fertil Steril 2013;99(1):37-43.
Savasi V, Mandia L, Laoreti A, et al. Reproductive assistance in HIV serodiscordant couples. Hum Reprod Update 2013;19(2):136-150.
Speroff L, Fritz MA. Clinical Gynecologic Endocrinology and Infertility, 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2010.
Twisk M, Mastenbroek S, van Wely M, et al. Preimplantation genetic screening for abnormal number of chromosomes (aneuploidies) in in vitro fertilization or intracytoplasmic sperm injection (review). Cochrane Database Syst Rev2006;(1 ):CD005291.
More on the topic 35 Infertility and Assisted Reproductive Technologies:
- REFERENCES
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- References
- Prevention of endometriosis
- Management of Fetal Growth Pathology in Multiple Pregnancy
- 37 Uterine Leiomyomas
- Contributors