Structural abnormalities
Since the introduction of routine ultrasound scanning as part of the antenatal care in the 1980s, there has been a continuous development of both the technology as well as the knowledge and experience of the clinicians.
The prevalence of fetal structural abnormalities is approximately 2% with congenital malformations accounting for 20% of the neonatal deaths.
Cardiac defects are perhaps the most common abnormalities encountered in approximately 5-10 out of every 1000 births. The second most common defects are abnormalities of the central nervous system with an incidence of 5:1000 of neural tube defects.
Detection in the first and second trimester using ultrasound
Currently, there are two ultrasound examinations offered to all pregnant women, each with different aims. The first trimester ultrasound is performed between 11 and 14 weeks of gestational age. The primary objectives are confirmation of viability, dating the pregnancy accurately according to the CRL, and to offer screening for common chromosomal abnormalities. The technological advances in ultrasonography have improved resolution and capabilities to such an extent that it has changed our understanding and ability to visualize early fetal anatomy. In doing so, structural abnormalities are being detected at an earlier stage, allowing for early counselling and intervention when required. This is the case for lethal malformations such as anencephaly, holoprosencephaly, and body-stalk anomaly. Other malformations that can be detected in the first trimester are defects of the anterior abdominal wall (gastroschisis, exomphalos), congenital diaphragmatic hernia, and megacystis.
The second ultrasound scan is performed between 18 and 21 weeks. The purpose of this scan is to identify major fetal structural abnormalities. The NHS FASP has identified 11 structural abnormalities with anticipated detection rates of greater than 50%, that should be routinely screened for (Table 11.1).
Although some other conditions can be detected during the anomaly scan, there is insufficient published data on detection rates to establish a standard. If any of these or any other abnormality is suspected, a referral to aTable 11.1 Screening for fetal structural abnormalities
| Abnormality | I Expected detection rate (%) |
| Anencephaly | 98 |
| Open spina bifida | 90 |
| Cleft lip | 75 |
| Diaphragmatic hernia | 60 |
| Gastroschisis | 98 |
| Exomphalos | 80 |
| Serious cardiac abnormalities | 50 |
| Bilateral renal agenesis | 84 |
| Lethal skeletal dysplasia | 60 |
| Edward syndrome (trisomy 18) | 95 |
| Patau syndrome (trisomy 13) | 95 |
fetal medicine unit should be made to confirm diagnosis and offer appropriate management. Identification of any malformation at this stage allows the parents to make decisions regarding continuation of pregnancy, and if the pregnancy continues, appropriate management with intervention or supportive care if required (antenatal or in the early postnatal period). Table 11.1 shows the anticipated prenatal detection rates of these 11 structural abnormalities.
The FASP committee has established a series of routine views, measurements, and images that should be obtained and stored during the anomaly scan. It is important to have a systematic approach when examining the fetus. Before starting the fetal biometry, it is advisable to examine the uterus and its contents, the fetal position, and orientation within the uterine cavity, confirming viability, number of fetuses, and chorionicity in multiple pregnancies.
In addition, it is essential to assess the amniotic fluid volume and the placental site as well as its structure. Once this has been established, the sonographer should proceed with fetal biometry. The standard measurements that should be obtained are as follows:1. Head circumference (HC). This can be measured in a thalamic plane (as established by the International Society of Ultrasound in Obstetrics & Gynecology Education Committee guidelines) (31) or in a transventricular plane (NHS FASP) (3). The landmarks are the CSP, the thalami, and the posterior lateral ventricles. It can be measured by placing an ellipse directly around the outside if the skull bone or by measuring the biparietal diameter and the occipitofrontal diameter and calculating the HC (Figure 11.3).
2. Abdominal circumference (AC). This is measured on a transverse plane of the abdomen. The landmarks of the AC plane are the stomach, the umbilical vein at the level of the portal sinus, and one entire rib should be seen (Figure 11.4). The AC may be measured placing an ellipse or measuring the anteroposterior abdominal diameter and the transverse abdominal diameter placing the callipers from the skin covering the abdomen.
3. Femur length (FL). The landmarks to measure the FL are an angle of insonation of 30 degrees, both ends of the ossified diaphysis, and tissue beyond them needs to be seen (Figure 11.5).

Figure 11.4 Transverse section of the fetal abdomen showing measurement of the transverse abdominal diameter (TAD) and the anteroposterior diameter (APAD) to obtain the abdominal circumference (AC).
These measurements need to be plotted on appropriate charts according to gestational age. If the pregnancy has not been previously dated (according to CRL in the first trimester), this needs to be done according to the HC and documented in the report.
A systematic examination of fetal anatomy needs to include the following:
1.
Skull, brain, and spine. Shape and ossification of the fetal skull. In the brain, measures of the atrium of the posterior horn of the lateral ventricles, transcerebellar diameter, cisterna magna, and nuchal fold. The anatomy of these structures and the presence of the CSP need to be assessed. The spine is examined in three planes, coronal, sagittal, and transverse, allowing spina bifida, scoliosis, and agenesis of the sacrum among other possible structural defects to be excluded.2. Face. The soft tissues are best assessed on a coronal plane to evidence the nostrils and lips. In the profile view, it is possible to assess the presence of a nasal bone and the shape of the maxilla and chin. Transverse planes are needed to assess the orbits and the alveolar ridge.

Figure 11.3 Transventricular plane of the fetal head showing measurement of the biparietal diameter (BPD), occipitofrontal diameter (OFD), and posterior ventricular atrium (Vp).

Figure 11.5 Femur length.
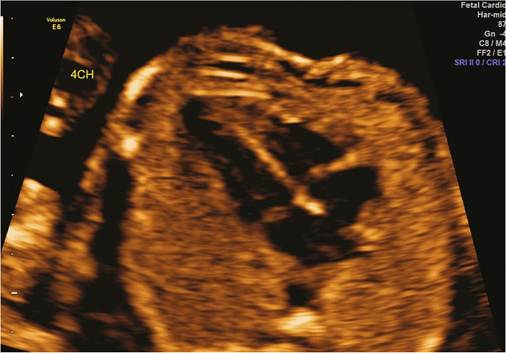
Figure 11.6 Four-chamber view of the heart.
3. 'Thorax. Examination of the lungs (uniform echogenicity), ribs (ossification, shape, number), and the integrity of the diaphragm. The diaphragm can be assessed on a sagittal plane as an echolucent line separating the thorax from the abdomen. The presence of the stomach in the thorax should raise the suspicion of congenital diaphragmatic hernia.
4. Heart. Basic routine examination of the heart includes three views: a four-chamber view, the left outflow tract arising from the left ventricle, and the three-vessel view showing the right outflow tract, the aorta, and the superior vena cava. The four- chamber view is obtained on a transverse plane and allows examination of the integrity of the interventricular septum, the morphology and size of both atria and ventricles, the atrioventricular valves moving freely and their insertion, and the foramen ovale moving in the left atrium (Figure 11.6).
5.
Abdomen. Examination of the abdomen in a transverse section allows visualization of the stomach bubble at the level used to measure the AC. Moving caudally, the insertion of the umbilical cord in the abdominal wall must be evidenced to assess its integrity. At the same level, the bowels should have uniform echogenicity and no sign of dilatation in the second trimester.6. Urinary tract. The kidneys are best visualized on a transverse view lower than the plane used for the abdomen. They appear like two rounded structures on both sides of the spine. In this view, it is possible to examine and measure the renal pelvises to exclude hydronephrosis. The fetal bladder is seen on a transverse section of the pelvis. The two arteries in the umbilical cord can be seen with colour Doppler on both sides of the bladder.
7. Limbs. All four limbs need to be assessed. In the lower limbs, it is important to confirm the presence of all long bones (femur, fibula, and tibia) and the angle of the leg with the foot to assess the presence of talipes. In the upper limbs, similarly, the presence of all long bones (humerus, radius, and ulna). In addition, the five metacarpals and five metatarsals in the hands and feet respectively and the density, length, and shape of bones need to be assessed.
8. Genitalia. Examination of the genitalia is not part of the routine fetal anomaly scan but it is good practice to assess normal anatomy especially if other structural abnormalities have been diagnosed.
Common structural abnormalities
Central nervous system
Neural tube defects arise from abnormal closure of the neural folds in the third and fourth weeks of development. They can involve the meninges, vertebrae, muscles, and skin. Neural tube defects include anencephaly, encephalocoele, and spina bifida. The incidence is about 5:1000 births in the United Kingdom with the majority being spina bifida (95% of cases).
Anencephaly is the absence of the cranial vault. Ossification of the fetal skull is normally complete by 11 weeks' gestation.
At the end of the first trimester, the absence of the cranial bones (acrania) may be noted which allows early diagnosis and management. It is a lethal condition and the majority of patients opt for termination of pregnancy.Encephalocoele is a defect in the cranium, which results in the herniation of a sac containing either fluid or part of the brain. The most common location is in the occipital region. The prognosis depends on the degree of herniation and the integrity of the underlying brain. In view of this, the parents may opt to terminate the pregnancy. Some cases are associated with Meckel-Gruber syndrome. The inheritance is autosomal recessive, and therefore the recurrence risk is one in four. Genetic referral is advised for further counselling.
In spina bifida, the defect is in the neural arch and is most commonly seen in the lumbosacral region. The spinal defect may be identified during the examination of the spine in lateral and transverse views by an interruption on the skin covering the spine and the presence of a myelocoele or a myelomeningocoele. Two additional cranial signs of spina bifida have been described: the ‘lemon sign', defined as a deformity in the frontal bones seen between 16 and 24 weeks, and the ‘banana sign', referring to the characteristic shape of the cerebellum that can be seen from 15 weeks (32).
Ventriculomegaly occurs in 1% of pregnancies and refers to the enlargement (diameter >10 mm) of the posterior lateral ventricles. The severe form, hydrocephalus, is often associated with other defects such as spina bifida (Figure 11.7).
Holoprosencephaly consists of several disorders characterized by the incomplete cleavage of the forebrain. It occurs in 1:10,000 pregnancies and can be associated with facial clefts and trisomy 13.
Face
The commonest facial abnormalities seen on ultrasound are cleft lip and palate. However, the antenatal detection rate is 30-35% at best. The face needs to be examined in sagittal, transverse, and coronal planes by ultrasound. In 75% of cases the abnormality is unilateral with the left side affected more often. It is important to be aware that there is a close relationship between midline facial clefts and abnormalities of the forebrain such as holoprosencephaly. The FASP aims at improving the detection of cleft lips and palates.
Cardiac defects
Congenital cardiac defects are one of the commonest fetal malformations occurring in 5-10:1000 live births. There is a huge regional variation in the prenatal detection rates of cardiac abnormalities by ultrasound ranging from 16.7% to 94% for major abnormalities. However, prenatal diagnosis of cardiac defects can improve significantly the outcome of the pregnancy. This is particularly true in the case of transposition of the great arteries, hypoplastic left heart

Figure 11.7 Ventriculomegaly, borderline measurement 10.6 mm.
syndrome, and coarctation of the aorta. Basic examination of the fetal heart should include the four-chamber view and ventricular outflow tracts. The detection rate of congenital heart disease is increased from 48% to 78% with the addition of the outflow tracts to the four-chamber view. If an abnormality is suspected, a fetal echocardiogram should be offered.
Thorax
The most common thoracic anomaly is congenital diaphragmatic hernia. The defect on the diaphragm allows the abdominal contents to shift into the thorax and the stomach may be visualized on the same plane as the heart that may be shifted to the right. The incidence is in 1:4000 pregnancies with 85% of cases occurring on the left side. The prognosis is worse if there is herniation of the fetal liver. The most commonly associated chromosomal abnormality is trisomy 18. Complications for the fetus arise from pressure on the heart and lungs causing mediastinal shift, pulmonary hypoplasia, pulmonary hypertension, and rarely hydrops.
Other malformations found in the chest are pleural effusions, cystic lesions of the lung, the most frequent one being congenital cystic adenomatoid malformation (CCAM) and less frequently bronchogenic cysts, lung sequestration, and bronchial atresia. The CCAM occurs in 1:4000 births. The condition may be bilateral involving all lung tissue, which is a lethal condition, or unilateral confined to a single lobe. The lesions are described as macrocystic (cysts >5 mm) or microcystic (cysts of a national or recommended policy on screening for abnormalities, the service was not always delivered. Responsible factors were lack of resources, lack of uptake, or late booking—the latter two influenced by social and cultural factors.
Although the detection of fetal anomalies is enhanced by ultrasound, any beneficial effect is far from proven. The Helsinki ultrasound trial in 1990 showed that the perinatal mortality was significantly lower in the group screened with ultrasound, and that a 49% reduction in the perinatal mortality was achieved due to early detection of abnormalities and the termination that followed. This contrasted with the findings of the RADIUS trial that showed the perinatal outcome and the frequency of induced abortion was unchanged with or without routine ultrasound screening. Both these studies were published more than 20 years ago. Since then, there have been significant improvements in equipment quality and training as well as knowledge of operators performing the screening. Even in the absence of robust evidence based on randomized controlled trials, routine ultrasound screening is now established as part of antenatal care (35).
Ultrasound is an established practice in the prenatal diagnosis of structural abnormalities in developed countries. As the standard of practice varies widely, many countries such as the United Kingdom are adopting national programmes in an attempt to improve the quality of service for all pregnant women. The management of women diagnosed with a fetus with a structural abnormality requires a multidisciplinary approach. The aim is to provide the required information, support, and time to enable parents to decide how they wish to manage the pregnancy.
More on the topic Structural abnormalities:
- Screening for chromosomal abnormalities
- Diagnostic procedures
- Chromosomal abnormalities
- Invasive Prenatal Diagnosis in Multiple Pregnancy
- REFERENCES
- External cephalic version
- Ultrasound-guided fetal therapy
- Chorionicity and zygosity
- Chapter 14 Fetal Growth Abnormalities: Intrauterine Growth Restriction and Macrosomia
- I AMENORRHEA