CARDIOMYOPATHIES
Although myocardial functions are commonly impaired in congenital, valvular or coronary diseases, the term cardiomyopathy (CM) is used to denote rare primary diseases of the heart muscle, excluding abovementioned causes.
Overall prevalence of cardiomyopathy is ~10 per lac live births.TABLE 17.32: Causes of dilated cardiomyopathy
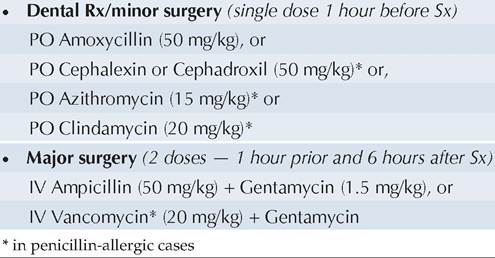
Fig. 17.23: Dilated cardiomyopathy.
Cardiomyopathies are broadly classified as:
• Dilated or congestive CM, the commonest type, with decreased contractility and consequent dilatation of ventricles.
• Hypertrophic CM, with inappropriate left ventricular hypertrophy, but normal ventricular contractility.
• Restrictive CM, with ventricular endocardial scarring and consequently reduced diastolic filling.
Dilated cardiomyopathy (DCM) is characterized by massive cardiomegaly involving all chambers, mainly LV. Decreased contractility of ventricles leads to stasis of blood flow and intracavitary thrombus formation. Histology reveals extensive foci of myocardial degeneration, necrosis and fibrosis, but without inflammatory cells.
Etiology: Though mostly idiopathic, DCM may be familial (20-50%), post-infectious or due to other causes (Table 17.32).
Clinically, DCM presents at any age with variable manifestations, e.g. (a) asymptomatic cardiomegaly, (b) failure to thrive, (c) early signs of LVF, e.g. ill-sustained breast-sucking in infants or exertional dyspnea in older children, or (d) CCF, usually precipitated by mild infections or other stress.
Common cardiac finding include—(a) LV apical impulse, displaced outward and downward, (b) muffling of heart sounds (c) gallop rhythm, and (d) soft systolic murmur due to valvular ring dilatation (MR/TR).
Investigations: Chest X-ray reveals cardiomegaly with/ without pulmonary edema (Fig. 17.23). ECG may show sinus tachycardia, rhythm abnormalities, evidence of LVH with or without ST segment/T wave changes and features of LA or RA enlargement.
Echocardiography is diagnostic, with gross dilatation and poor contractility of ventricles, mainly LV. Pericardial effusion and intracavitary thrombus may be seen
Cardiac catheterization, though rarely needed, demonstrates LV dysfunction, reduced cardiac output, valvular regurgitation and increased left-sided filling pressures. Treatment is mainly supportive, with—(a) restriction of strenuous activity, (b) aggressive management of CCF with diuretics and digoxin, (c) after-load reduction with vasodilators, e.g. ACE inhibitors, (d) inotropic support with dobutamine/dopamine, and (e) anti-arrhythmic agents, if required. #946;-blockers have been found effective in some cases.
Anticoagulant therapy (coumadin or heparin) is indicated in cases with recurrent intraventricular thrombus formation. Cardiac transplantation is the only definite mode of therapy.
Prognosis: DCM is usually progressive, with complications, e.g. arrhythmia and thromboembolic episodes being terminal events.
Hypertrophic cardiomyopathy (HROM) is relatively uncommon, characterized by massive LVH but well- preserved contractile function. The ventricular cavity may be normal or small in size. Poor compliance of hypertrophied and fibrosed muscle leads to impaired diastolic ventricular filling, gt; LA enlargement, and gt; pulmonary venous congestion due to back-pressure. LV outflow obstruction may develop in few cases.
Histopathological features are typical, with gross disorganization of the muscle bundles (Whorl pattern), disorganized myofibrillar architecture and marked fibrosis.
Etiology: HROM is usually an autosomal dominant disease, involving mutations of the genes encoding cardiac #946;-myosin heavy-chain and myosin-binding protein C.
Secondary HROM may develop in cases with LV outflow obstruction, e.g. coarctation of aorta/critical aortic stenosis and mucopolysaccharidosis.Clinically, it is more common in adolescents and young adults, presenting with signs of reduced LV output, e.g. weakness, fatigue, exertional dyspnea, palpitation, dizziness, syncope and sometimes anginal pain due to coronary obstruction.
On examination: (a) Pulse is brisk due to the early systolic ejection of blood from the ventricle, (b) Apex beat is forceful, heaving and displaced laterally suggestive of LV pressure overload, and (c) Ejection systolic murmur is audible at the lower sternal border or apex, which increases in erect posture or during Valsalva maneuver (unlike most other murmurs, which usually reduce in intensity/duration on these activities).
Investigations: Chest X-ray shows mild LV cardiomegaly with normal pulmonary vasculature. ECG abnormalities include LVH, ST segment/T wave charges, deep Q waves and absent/diminished R waves in the left precordial leads.
Echocardiography is diagnostic, showing—(a) LVH encroaching the interventricular septum, (b) small LV cavity, and (c) narrowed LV outflow tract. M-mode echo demonstrates asymmetric septal hypertrophy of the interventricular septum and occasional systolic antimotion of the anterior mitral valve leaflet.
Cardiac catheterization is useful before surgical intervention, to assess the LV compliance, presence of MR and dynamic LV outflow gradient.
Treatment can be medical or surgical.
Medical treatment includes—(a) avoidance of strenuous physical activity, (b) #946;-blockers, e.g. Propranalol to decrease anginal pain, arrhythmias and outflow obstruction, (c) calcium-channel blockers, e.g. nifedipine to improve diastolic filling and decrease hypercontractile systolic functions, (d) diuretics to reduce congestive symptoms, and (e) endocarditis-prophylaxis, prior to surgical interventions. Digitalis is contraindicated and may increase the degree of obstruction.
Surgical treatment, i.e. ventricular septal myotomy with/without mitral valve replacement is indicated in non-responsive cases with disabling angina/ syncope or severe obstruction (pressure gradient gt; 50 mm Hg).
Periodic family screening with ECG/echocardiography is advisable even in asymptomatic siblings for early diagnosis of disease.
Prognosis is unpredictable and obstruction may be stable or slowly progressive. Common complications include arrhythmias and infective endocarditis.
Restrictive cardiomyopathy (RCM) is least common, characterized by impaired diastolic filling due to excessively rigid ventricular walls.
Etiology: RCM is usually secondary to hemosiderosis, hemochromatosis, endomyocardial fibrosis, hyper- eosinophilic syndrome and collagen vascular diseases, etc. Clinically, exercise intolerance is the commonest presentation of RCM, as the cardiac output cannot be increased beyond a certain limit due to compromised ventricular filling. Other symptoms include weakness, dyspnea and chest pain.
Examination usually mimics constrictive pericarditis with raised JVP, pedal edema, hepatomegaly and Kussmaul's sign, i.e. paradoxical increase in JVP during inspiration.
Investigations: Chest X-ray is usually normal or reveals mild cardiomegaly and pulmonary venous hypertension. ECG may show the presence of atrial fibrillation or AV conduction defects.
Echocardiography is characteristic, revealing 'bi-atrial enlargement with normal cavity size of both ventricles'. LV systolic function is affected only in late stages.
Cardiac catheterization reveals characteristic “squarerootquot; sign in the ventricular pressure recordings, with
reduced ventricular compliance and increased filling pressures.
Treatment: Digoxin is not indicated as the Systolicfunction is unimpaired. Diuretics offer some benefit. Anticoagulants and antiplatelet agents may be used for prevention of thrombosis and a pacemaker may be used for management of complete heart block.
Role of steroids and immunosuppressive agents is yet to be defined. Cardiac transplantation is an option, worth considering.Endocardial Fibroelastosis
Endocardial fibroelastosis (EFE) is a rare cardiac disorder, pathologically characterized by white, opaque, fibroelastic thickening of the endocardium, usually involving LV.
Etiologically, EFE may be primary isolated abnormality or secondary to severe Left-sided obstructive CHD, e.g. aortic stenosis/atresia or coarctation of aorta. Although association is uncertain, primary EFE has been associated with prenatal/postnatal mumps infection.
Clinically, most cases present within first 6 months of life, with acute CCF following mild respiratory infection or with features of chronic heart failure, e.g. recurrent chest infections and failure to thrive.
Diagnosis is supported by—(a) cardiomegaly on X-ray, (b) LVH with strain pattern on ECG and (c) bright appearing endocardial surface with poorly functioning LV on echocardiography.
Treatment is mainly palliative, to control CCF with digitalis and diuretics. Most cases eventually succumb in early childhood unless heart transplant is possible.
17.9
More on the topic CARDIOMYOPATHIES:
- Myocardial Cytokine Expression as a Factor in Cardiomyopathy
- Myocarditis and Viral Myocardial Infection as Causes of Cardiomyopathy
- REFERENCES
- Macrovascular Complications of Diabetes Mellitus
- CMR of Myocarditis
- CONGESTIVE CARDIAC FAILURE
- Constrictive Pericarditis
- Prepregnancy counselling
- Polyarteritis Nodosa
- Ischemic Heart Disease