NEONATAL RESUSCITATION
While most newborns do not require any resuscitation beyond the maintenance of temperature, suctioning of airways and mild stimulation, adverse perinatal events, e.g. birth asphyxia may preclude smooth neonatal cardiopulmonary transition, unless assisted.
TABLE 12.6: Placental exam and its significance
TABLE 12.7: Resuscitation alert (high-risk delivery)
Normal
Placental weight : 400-500 gm
Umblical cord length : 30-50 cm
Abnormal placenta
• Large size: IU infections, polyhydramnios, Rh-HDN
• Small size: IUGR, maternal malnutrition
• Type: Monozygous vs Dizygous (in twins)
• Dull/milky: IU sepsis
• Grayish/yellow: Meconium deliveries, Rh-HDN
• Nodular: Oligohydramnios
• Multiple infarcts: IU hypoxia, post-maturity
• Retroplacental hemorrhage: Severe anemia
• Histological examination for tubercles, malaria
IUGR: Intrauterine growth retardation, Rh-HDN: Rh-hemolytic disease of newborn
• High-risk pregnancy (Table 12.2)
+
• Pre-term/post-term delivery
• Malpresentation, e.g.
breech, transverse, etc.• Obstructed/prolonged labor
• Signs of fetal distress:
- Meconium stained liquor amnii
- Altered fetal heart sounds/movements
- Abnormal tests for fetal well-being, e.g. NST
• Premature rupture of membranes
• Cord prolapse
• Cord around the neck
• Interventional delivery: LSCS, forceps, etc.
• Low Apgar score at 1 minutes (lt;4)
NST: Non-stress test
Primary goal of neonatal resuscitation is to establish adequate respiration and cardiac output in asphyxiated newborns at birth, to prevent early neonatal morbidity/ mortality as well as late sequelae of hypoxic-ischemic damage.
Pathophysiology: Asphyxiated babies, whether in utero or post-birth, respond to the oxygen deprivation in a fairly constant sequence, i.e. development of primary apnea followed by terminal apnea.
Primary apnea is the immediate and transient response to oxygen deprivation, usually preceded by a short period of rapid breathing, followed by sudden cessation of breathing, falling heart rate (usually gt;100/ min) but with maintained blood pressure. These cases respond well to gentle tactile stimulation with re-initiation of breathing.
Terminal apnea is the response to continued asphyxia, after a brief period of recovery from primary apnea, characterized by gradual cessation of breathing after few gasps with significant drop in heart rate (lt;100/min), blood pressure and unresponsiveness to stimuli. These patients do not respond to tactile stimulation and need more intensive resuscitation.
In cases of fetal hypoxia, one or both phases may pass in utero and the baby may be born in primary or terminal apnea, which is difficult to distinguish and it is safer to assume that s/he is terminal apnea and needs full resuscitation.
Other important considerations in resuscitation of newborns are:
• High airway resistance and pulmonary vascular resistance, due to poor lung expansion in first few breaths,
• Consequent hypoxia and acidosis leading to poor pulmonary perfusion and myocardial dysfunction, and
• Redistribution of blood flow from non-vital to vital organs (diving-in reflex) leading to multi-organ dysfunction.
Resuscitation alert: Although the need for resuscitation may arise unexpectedly, it is often possible to identify high-risk cases on the basis of proper history, review of previous maternal records and monitoring of the obstetrical course (Table 12.7).
Pre-delivery preparations: All high risk deliveries must be attended by an adequately-trained pediatrician, preferably with an assistant. As soon as the need for neonatal resuscitation is felt, a pre-arranged plan of action should be activated to ensure presence of the trained staff and availability/ functioning of resuscitation equipment/drugs, etc. (Table 12.8).
TABLE 12.8: Resuscitation equipments and drugs
• Pre-warmed resuscitation tray
• Pre-warmed warmer/resuscitation trolley
• Suction equipments
- Low-pressure suction machine
- Delee' mucus extractor
- Suction catheter 10,12,14 Fr.
• Oxygen source with humidification and flow gauze
• Bag and mask ventilation
- Resuscitation (AMBU) bag ( 250-500 ml)
- Neonatal face masks
• Intubation equipments
- Laryngoscope with straight blades (size 0, 1)
- Endotracheal tubes (size 2.5, 3, 3.5, 4) with adopter/stylet
- Nasogastric tube
• Medications
- Umbilical catheters 3.5-5 Fr
- Syringes and needles
- Pre-filled Adrenaline (1:10000)
- IV fluids: Normal saline
- Naloxone hydrochloride
• Others
- Timer
- Linen/ gauze
- Gloves
• Working electrical points
• Adequate manpower
TABLE 12.9: TABC of neonatal resuscitation
Temperature control
• Warmth under radiant warmer
• Drying the baby
• Removal of wet linens
Airway patency by
• Proper positioning
• Oropharyngeal suction
• Endotracheal suction
Breathing by
• Tactile stimulation
• Positive pressure breathing (PPV)
• Endotracheal intubation
Circulation by
• Chest compressions
• Medications
Principles: Basic principles of neonatal resuscitation include measures to restore and maintain four cardinal body functions—temperature, airway, breathing and circulation, often referred as TABC of resuscitation (Table 12.9).
Protocol: Current neonatal resuscitation program (NRP), based on American Academy of Pediatrics recommendations 2020, propose a step-wise algorithm, as follows (Fig. 12.1):
Step I. Initial assessment, as soon as the baby is delivered, aims to identify babies who need resuscitation, based on three simple parameters: (a) gestation, (b) tone, i.e. posture and movements, and (c) breathing or crying. No further resuscitation is required if the baby is full term, breathing/crying and moving with flexed posture, except basic delivery room care (Ch 12.4.1).
Babies who are preterm, flaccid or not breathing/ crying, need immediate resuscitation with following steps. In them, cord should be clamped and cut as soon as possible, without waiting for minimum 30 seconds (Early cord clamping).
Step II. Initial steps in resuscitation aim to prevent hypothermia, clear the airways and stimulate breathing, by following interventions termed “initial steps”, which should be completed within 30 seconds.
a. Warm: Place the baby under a radiant warmer.
b. Dry with pre-warmed linens and remove wet linens.
c. Stimulate by gently rubbing the trunk, back and extremities to stimulate breathing/crying. Do not shake or rub vigorously.
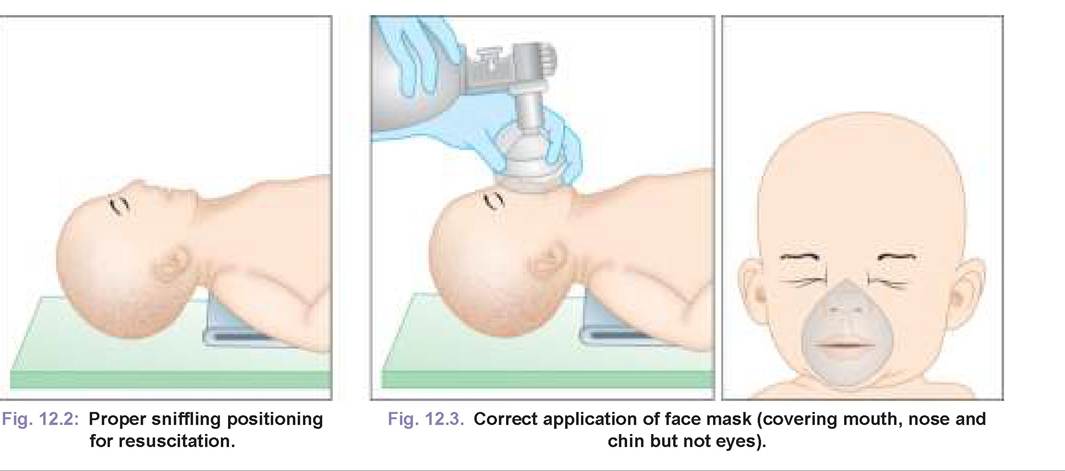
d. Position the baby in supine position with neck slightly extended (sniffling position) to bring posterior pharynx, larynx and trachea in line and facilitate breathing. To maintain this position, a rolled towel may be placed under the shoulders (Fig. 12.2).
e. Clear airway by wiping of the nose/mouth, though a gentle suction with a disposable mucus extractor or a 12-14 Fr. catheter may be required to clear the airway in some newborns. Head may be turned to one side
to clear secretions in babies with copious secretions.
Essentials of a good suction are as follows:
- Mouth should be suctioned before the nose (M before N);
- Suction pressure should never exceed 100 mm Hg (130 cm H2O);
- Suction catheter should not be inserted too deep, to avoid vagal stimulation and
Intrapartum suction or postnatal tracheal suction in non- vigorous babies with meconium stained amniotic fluid is no longer recommended.
Step III. Re-evaluation: After initial steps, baby must be re-assessed at 30 seconds. Approximately 60 seconds (“the Golden Minute”) are allotted for completing the initial steps, re-evaluation and beginning the breathing support, if required.
Current guidelines recommend use of two parameters-heart rate (HR) and respiration at 30 seconds, to decide further resuscitation measures, as well as observation for color or monitor for target SpO2 (Fig. 12.1).
Auscultate the heart or palpate for cord pulsations to assess the HR, which should be counted for 6 seconds multiplied by 10 to arrive at HR/min.
Simultaneously, color should be observed over mucus membranes, e.g. tongue to detect central cyanosis (acrocyanosis has no significance in resuscitation).No further intervention is required in babies with HR gt;100 and breathing normally, except to ensure warmth, clear airways and monitoring. Other cases need further resuscitation as follows:
- Babies with labored breathing and/or persistent central cyanosis must be provided supplemental oxygen at the rate of 5 L/min with a face mask, along with SpO2 monitoring.
- Babies with: (a) apnea or gasping respiration, (b) HR lt; 100 or (c) persistent cyanosis on 100% oxygen must be started on positive pressure ventilation without delay (within the golden minute).
Step IV. Positive pressure ventilation (PPV) should be initiated without delay for indications as above, using a self-inflating resuscitation bag (ambulatory breathing unit or AMBU bag) with face mask (Fig. 12.3). Resuscitation bag usually delivers 21% oxygen at room air without oxygen connection, 40-50% at an oxygen flow rate of 4-5 L/min with no reservoir, and 90-100%, if used with a reservoir. PPV is contraindicated in cases with diaphragmatic hernia, but may be used in those with potential meconium aspiration.
Some important considerations for bag and mask ventilation in NRP are as follows:
• Appropriate position of the head with slight extension to ensure clear airways.
• Appropriate size of resuscitation bag (250-500 ml)
Fig. 12.1: Neonatal Resuscitation Algorithm.
Adopted from: American Heart Association 2020 guidelines.
• Appropriately fitting face mask to cover the nose and mouth but not the eyes.
• Appropriate FiO2 with room air in babies gt;35 weeks and 21-30% for preterms lt;35 weeks, though should be adjusted later according to SpO2 monitoring for target values, to the maximum of 100% in case of no improvement in 90 seconds.
• Appropriate ventilation pressure, applied by fingers and not the hands. First few breaths require higher bagging pressure (30-40 cm H2O) to expand collapsed lungs,
but subsequent pressure should not exceed 20-25 cm H2O, to prevent barotrauma.
• Appropriate ventilation rate of 40-60/min, following a squeeze, one, two three, squeeze... sequence.
• Successful bag and mask ventilation is indicated by:
(a) good chest rise, (b) symmetric air entry, (c) disappearance of cyanosis, and (d) increase in heart rate. In absence of these indicators with poor chest wall movement and absence of breath sound on auscultation, following reasons and Corrective steps should be considered: (a) inadequate seal (reapply mask), (b) blocked airways (reposition the head, clear secretions by suction, and ventilate with mouth slightly open), (c) inadequate pressure (increase pressure slightly).
• PPV may also cause gastric distension due to swallowed air, which can be prevented by insertion of an orogastric tube in stomach, if PPV is required for gt;2 minutes.
After 30 seconds of effective PPV, baby should be evaluated again for HR to make following decisions:
• Babies with HR gt;100/min should be continued on PPV with monitoring. As the spontaneous breaths start, rate must be reduced accordingly and PPV can be stopped when baby has good respiratory efforts with HR persistently gt; 100/min.
• Babies with HR lt;100 but gt; 60, who do not improve despite increasing FiO2 must be considered for endotracheal intubation.
Step V: Endotracheal (ET) intubation is indicated only in small proportion of cases, with: (a) poor response to PPV (HR lt; 100 and not increasing) after 30 seconds, (b) suspected diaphragmatic hernia, and (c) extreme preterm infants, who are also going to need surfactant therapy. Essentials of good ET intubation include:
• Appropriate size of laryngoscope blade, i.e. straightblade of size 0 (preterms) or 1 (term).
• Appropriate size of ET tube, i.e. 2.5 for lt;1 kg; 3 for 1-2 kg; 3.5 for 2-3 kg and 4 for gt;3 kg.
• Appropriate depth of ET tube, calculated as distance from tip of the nose to tragus + 1 cm.
• Appropriate skill to perform, with each attempt not exceeding gt;20 seconds. Intermittent bag/mask ventilation for 30 seconds must be given before the next attempt, to prevent hypoxia.
• Correct placement of the ETT must be confirmed by bilaterally equal air entry and chest movement.
A laryngeal mask may be considered as an alternative to ETl intubation in newborns gt;34 weeks, if it is not feasible or unsuccessful.
Persistent of HR lt;60 despite effective ET intubation needs to begin with chest compressions and consider medications.
Step VI. Chest compressions aim to improve mechanical pumping of the blood to vital organs, indicated if HR remains lt;60/min despite 30 seconds of PPV. Chest compressions should be stopped once HR exceeds 60/min.
Chest compressions help to mechanically pump blood to vital organs and restore some perfusion and should always be accompanied with PPV.
Chest compressions involve compressing the lower- third of sternum by two-finger technique or by thumb technique (Fig. 12.4), interspersed with PPV, at a ratio of 3:1 (90 compressions:30 breaths). Essential features of good chest compressions are:
• Compression rate: ~ 90/min (with PPV 30/min).
• Depth: ~ 1/3rd of chest's antero-posterior diameter.
• Relaxation time more than compression time.
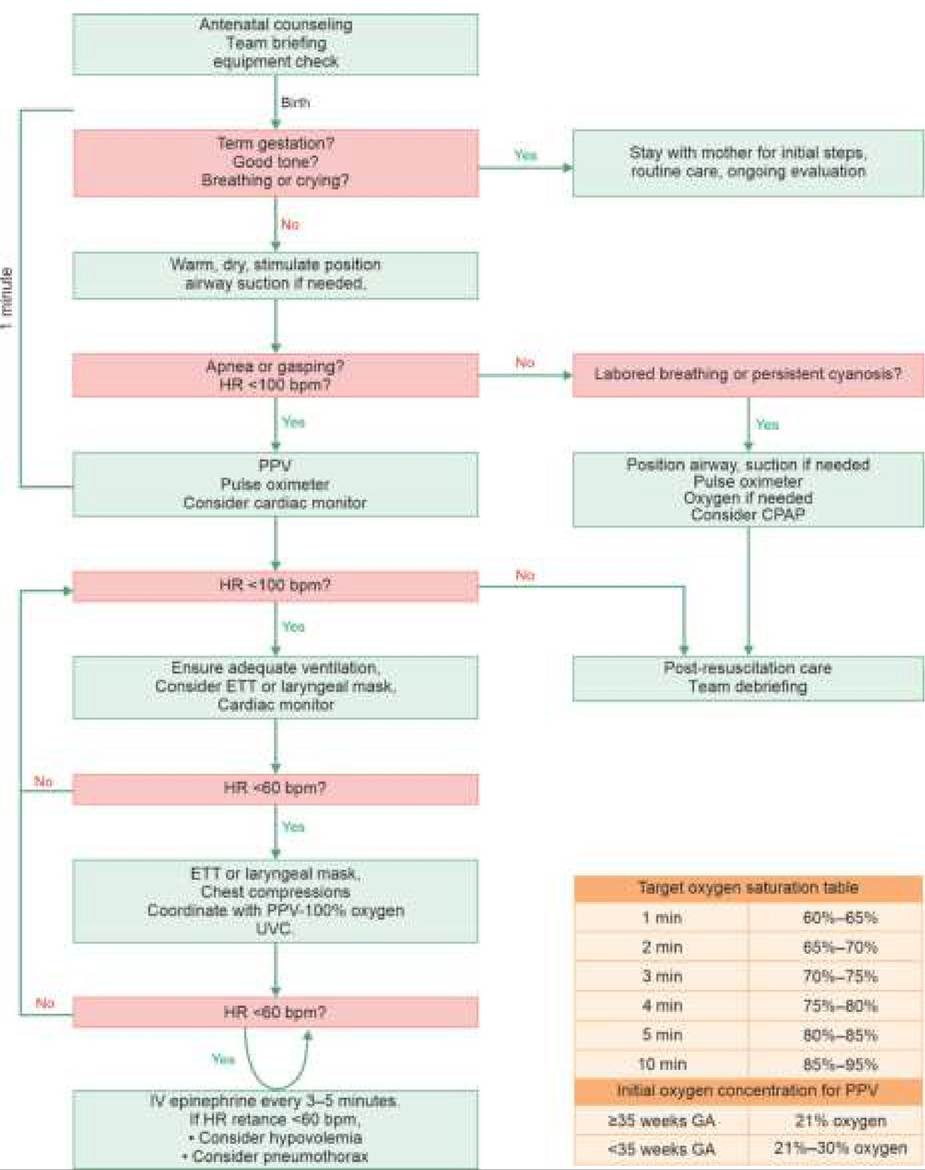
Fig. 12.4: External cardiac massage in newborns: (A) Two-finger technique; (B) Two-thumb technique.
Potential complications include rib fractures, pneumothorax and liver injury. Chest compressions should be discontinued once the HR exceeds 60/min, continuing with PPV at the rate of 40-60/ min.
Persistence of HR lt; 60 despite 60 seconds of chest compressions ad effective PPV, indicates need for medications.
Step VII. Medications have limited role in resuscitation, except epinephrine and volume expanders in some cases. Umbilical vein cannulation is preferred for quick IV access to deliver these medications, as follows:
• IV Adrenaline (1:10000) 0.1-0.3 ml/kg, is indicated if HR remains lt;60/ min after 60 seconds of effective PPV and chest compressions and may be repeated every 3-5 minutes. It may also be given intratracheally after diluting in 1-2 ml of normal saline, if IV access is not available.
• IV normal saline or Ringer lactate 10 ml/kg, as volume expander in newborns with hypovolemic shock (feeble peripheral pulses despite adequate HR and ventilation).
There is no role of atropine, naloxone and steroids etc during neonatal resuscitation.
Step VIII. Consolidation phase, after initial recovery, involves shifting the newborn to intensive care unit, gradual weaning from respiratory support and correction of fluid, electrolyte and acid-base imbalance, apart from other supportive measures, e.g. antibiotics. Blood transfusion (O-negative, irrespective of baby's group), 10 ml/kg, is indicated in babies with significant peripartum blood loss. IV dopamine, 5-10 mg/kg/min is used in shock, if blood pressure cannot be sustained with volume expanders.
When to stop resuscitation? It is a highly ethical and controversial issue though general consensus suggests futility of continued efforts in absence of heart rate for 20 minutes despite all appropriate steps in resuscitation were performed. Vigorous resuscitation is also not favored in: (a) extreme preterms lt;22 weeks or 500 gm,
TABLE 12.10: Apgar scoring system
Score
*Upper limbs flexed, lower limbs extended
or (b) presence of lethal anomalies, e.g. anencephaly. However, decision must be individualized on contextual factors.
Apgar score: Apgar scoring system, devised by an anaesthetist nurse Ms. Virginia Apgar, is the most popular evaluation tool to assess cardiopulmonary status at birth. Acronym APGAR stands for five evaluation parameters-Appearance (color), Pulse (HR), Grimace (reflex response to nasal catheter), Activity (tone) and Respiration (RR).
Methodology: Apgar scoring involves assessment of these five parameters at 1 minute and 5 minute of age, on a scale of 0-2 with maximum score of 10 (Table 12.10). However, if 5-minute score is lt;7, then additional scoring is done every 5 minutes till 20 minutes.
Utility: Apgar scoring assists to:
• Identify the need for immediate resuscitation, based on 1-minute score.
• Predict the late neurological outcome in asphyxiated baby, based on 5-minute score.
Limitations: the value of 1-minute Apgar score as a resuscitation guide is limited due to following reasons:
• First score is recorded at 1 minute, though resuscitative efforts should not be delayed that long.
• It is unreliable in preterms, congenital neuromuscular disorders or maternal sedation.
• Parameters, e.g. HR, tone, color and reflex activity are themselves dependent on respiration and hence, hardly provide additional information.
• Acrocyanosis (peripheral cyanosis) is common in normal newborns and hence, full score of 10 is unlikely, even in healthy crying baby.
However, 5-minutes score is an excellent predictor of late neurological outcome in asphyxiated newborns.
12.5 EXAMINATION OF A NEWBORN
Neonatal examination is difficult to complete in one sitting. A newborn has to examined repeatedly for complete evaluation, though following examinations are essential in each case: (a) preliminary examination
at birth, (b) comprehensive examination on first day in wards, (c) daily or more frequent follow-up examinations till discharge, and (d) final examination on discharge.
I. Delivery Room Examination
Delivery room examination aims to identify: (a) immediate need for resuscitation, (b) major congenital anomalies, and (c) high-risk neonate in need of advanced neonatal care and includes:
• Review of maternal and obstetrical records
• Assessment for Apgar scoring and vital signs to decide the need for resuscitation.
• Search for congenital anomalies, including orifice count and patency check if required.
• Quick physical evaluation for gestational age, birth weight and genitals for gender assignment, and
• Examination of placenta and umbilical cord for anomalies.
These aspects have been discussed in previous Ch 12.4.1.
II. First Day Examination in Nursery/Postnatal Ward
First day examination in nursery aims to evaluate the newborn in toto, to: (a) ensure general well-being, (b) precise assessment of gestation age, (c) identify missed congenital malformations or warning signals for sick newborn.
Essential prerequisites of good neonatal examination in nursery include:
• Baby should be examined at least frac12; hour after feeding, when alert, comfortable and not crying.
• Nursery temperature should be comfortably warm (28-30°), and fans must be switched-off before unwrapping the baby.
• Examiner's hands should be washed properly for at least 2 minutes with an antiseptic soap and running water, dried and warmed by rubbing.
• A flexible approach is necessary in examination sequence. Traumatic examinations, e.g. patency checks or deep palpation should be deferred till inspection is complete.
A general protocol of neonatal examination in nursery includes:
I. Re-review of maternal/birth records for high-risk factors, e.g. infections, systemic illnesses, obstetric complications and drug therapy, which may affect the postnatal course of baby.
II. Anthropometry: For example, weight and length should be recorded on first day, preferably by electronic balance and infantometer respectively, while head circumference should be recorded after 24 hours, after disappearance of cranial molding.
At birth, a full term newborn weighs ~3 kg, measures ~50 cm and has a head circumference of ~33 cm. However, she/he loses up to 10% of birth weight (15% in preterms) during 1st week but regains it by 10th day (14th day in preterms). Subsequently, a newborn gain ~20-30 gm/day.
Low birth weight (lt;2.5 kg) or large for date (gt;3.5 kg) indicate specific problems in postnatal period (Ch 12.11). Birth length may be less in preterms, IUGR, chromosomal disorders and skeletal dysplasias.
III. Examination of vital signs, e.g. temperature, heart rate, respiratory rate, peripheral capillary filling and, blood pressure in selected cases.
• Temperature should be recorded by axillary digital thermometer. Normal neonatal temperature fluctuates between 36.5 and 37.4°C, with hypothermia as an important warning sign of sick newborn. WHO recommends that neonatal temperature should be recorded once a day in apparently healthy term babies, thrice a day in healthy LBW, 6-hourly in healthy VLBW lt; 2 kg and every 2 hourly in sick newborns. Use of mercury based rectal thermometers is no longer recommended.
• Heart rate (HR) in newborns fluctuates between 100 and 160/minute. Persistent tachycardia (gt;180) indicates CCF or arrhythmias, while bradycardia (lt;100) may be due to—(a) apneic episodes, (b) hypoxic-ischemic injury, and (c) maternal sedation.
• Respiratory rate (RR) in newborns is often irregular and varies from 30 to 60/minute. Common respiratory abnormalities include apnea, periodic breathing or respiratory distress.
• Peripheral capillary filling is a reliable indicator of hemodynamic status in newborns, assessed by blanching the heel and recording the time taken to recover its color. Delayed filling of gt;3 second is a bad prognostic sign.
• Blood pressure (BP) measurements are difficult and not essential in all newborns. BP may be assessed by flush method (Ch 17.12), though precise measurement requires Doppler studies. Normal neonatal BP is ~70-80 mm/50-60 mm Hg. While hypotension indicates circulatory shock, hypertension in newborn is usually due to: (a) renal anomalies, (b) renal artery stenosis, (c) severe coarctation of aorta, and (d) congenital adrenal hyperplasia.
IV. General physical examination needs to be more comprehensive than at-birth evaluation, conducted in a cephalocaudal direction (head-to-toe) to assess gestation age as well as identify minor/ major problems, as follows: • General appearance: A term newborn tends to assume in utero flexed posture and sleeps for gt;20 hours/day. Appearance includes: (a) posture/movements, (b) general activity, and (c) cry
Abnormal posture: Limpness or asymmetric movements indicate—(a) hypoxic-ischemic damage,
(b) CNS malformations, (c) neuromuscular disorders, (d) birth injuries or (e) pressure deformities in breech deliveries or oligohydramnios.
Abnormal activity: Persistently sluggish activity is a warning signal of sick newborn, usually due to hypoxia, sepsis, hypothermia and hypoglycemia. On the other hand, tremulousness or jitteriness, may indicate hypoglycemia, hypocalcemia or hypoxia.
Abnormal cry: Feeble/low-pitch cry indicates sick newborn, while high-pitch cry is common in kernicterus or hypoxic brain damage. Hoarse cry indicates birth trauma with vocal cord paralysis.
• Skin should be examined for its texture, color, vernix caseosa, lanugo, minor problems and major warning signals.
Vernix caseosa is a cheesy-white substance that covers the fetus till 34-38 weeks of gestation and the amount of vernix decreases with advancing gestation.
Lanugo are soft-fuzzy immature hair over body in preterms, which are gradually replaced by mature vellus hair with advancing gestation.
Skin in term newborn is shiny, pink, with vernix present only at creases and lanugo present only at upper back and dorsum of limbs.
Skin in preterms is thin and delicate, bright-red color, with plenty of vernix and lanugo over entire body. Pedal edema is also common.
Skin in post-terms is lusterless that peels or cracks at creases, and may be yellowish due to intrauterine passage of meconium.
Common benign skin abnormalities in newborns are discussed in Ch 12.7.
Important warning signals on skin include: (a) severe pallor/ plethora, (b) persistent/central cyanosis,
(c) deep icterus, (d) cutis marmoratus, i.e. pale-mottled skin suggestive of sepsis or hypothermia, (e) bleeding spots, e.g. petechiae or ecchymosis, due to birth injury or bleeding disorders, (f) sclerema, i.e. diffuse hardening of skin over cheeks, buttocks, extremities and bony prominences seen in hypothermia, sepsis and hypoglycemia, (g) generalized edema, e.g. hydrops fetalis, and (h) severe infections.
• Head must be examined for—(a) shape, (b) circumference, (c) soft-tissue abnormalities, and (d) fontanels and sutures.
Shape may be transiently deformed at birth, due to molding—overriding of cranial bones by vaginal pressure, which gradually disappears in a few days. Excessive molding indicates obstructed/prolonged vaginal delivery.
Head circumference of a normal newborn is ~33-35 cm, which should be recorded only after 24 hours of birth, after molding disappears. Small size indicates microcephaly or craniosynostosis, while macrocephaly may be familial or due to CNS malformations, e.g. congenital hydrocephalus, hydroencephaly, etc.
Soft-tissue abnormalities of scalp are usually benign, e.g. caput succedaneum or cephalohematoma (Ch 12.10.2). Craniotabes, i.e. ping-pong feel due to compressible skull-vault, is physiological in newborns. Large caput, cephalohematoma or lacerations over scalp may indicate significant birth injury.
Anterior fontanel at birth is open, soft, flat and pulsatile with diagonal size of lt;3 cm, while posterior fontanel is closed or admits only a tip of finger. Cranial sutures are open but in close approximation. Large fontanels or wide-sutures at birth indicate: (a) prematurity, (b) hydrocephalus, (c) hypothyroidism,
(d) osteogenesis imperfecta, etc. Small fontanels suggest microcephaly/craniosynostosis. A third fontanel between anterior and posterior fontanel, is not a true fontanel but a defect in parietal bones, occasionally present in normal newborns or Down syndrome.
• Face should be examined for dysmorphic features and asymmetry during cry.
Facial dysmorphism is an important indicator of chromosomal or genetic disorders and generally includes—low hair-line, low-set ears, pre-auricular tags, slanting eyes, epicanthic folds, hyper/hypo- telorism, depressed nasal bridge, micro/ retrognathia, cleft lip, etc.
Facial asymmetry on crying may be due to congenital hypoplasia of depressor angularis oris muscle or birth injuries (facial palsy, mandibular injury).
• Eye examination is difficult in newborns due to physiological photophobia, though most babies may open eyes on gentle rocking. A quiet and alert newborn may fix the vision on examiner's face and follow it for few degrees of sideway movements. Pupillary reflex is present from 28th week of gestation.
Common eye abnormalities include: (a) benign problems, e.g. conjunctival hemorrhage, nasolacrimal duct obstruction, transient discharge, etc.; (b) malformations suggestive of intrauterine infections or chromosomal disorders, e.g. microphthalmia, micro/ macrocornea, coloboma, cataracts, or cat-eye-reflex, etc.; and (c) conjunctivitis.
• Ears should be examined for—(a) shape, recoil and deformities, (b) otoscopic exam in select cases and (c) hearing by startle response to sudden sound. Term newborns have well-formed cartilaginous pinna with good elastic recoil, relatively short and straight external auditory canal, easily visible dull-grey tympanic membrane and good startle response.
Transient ear discharge is common during first few days due to retained amniotic fluid. In preterms, ear cartilage is under-developed with slow recoil. Important ear abnormalities include malformed/ low-set ears (chromosomal disorders), pre-auricular pits/tags (associated renal anomalies) and persistent discharge (otitis media), etc.
• Nose should be examined for dysmorphism and patency (by lubricated soft-rubber catheter, if required). Most newborns are obligate nose-breathers.
Common abnormalities include depressed nasal bridge (hereditary, chromosomal), and stuffiness (choanal atresia/stenosis, infection, postural, etc.)
• Oral cavity must be inspected for cleft lip/palate or benign problems, e.g. natal tooth.
• Neck is relatively short in newborns but with full movements. Neck injuries are common in breech/ transverse lie and may lead to torticollis or sternoCleidomastoid tumor (Ch 12.10.2).
Important neck abnormalities include webbing (Turner syndrome), mid-line mass, e.g. goiter, cystic hygroma, thyroglossal cysts, and Iateralized lesions, e.g. branchial cysts/sinuses.
• Chest must be examined for shape, size, breast nodules, rib-cage and respiratory movements. Neonatal chest is barrel-shaped with prominent xiphisternum. Chest circumference is lesser than head circumference at birth. Breast nodule is ~10 mm in fullterms, with well-defined areola.
Apart from benign problems, e.g. supernumerary nipples and mastitis neonatorum, also look for widespaced nipples (Turner syndrome), tender rib-cage (birth injury) and increased intercostal movements suggestive of respiratory distress.
• Spine in newborns is relatively straight and more flexible, which should be examined for neural tube defects or its stigmata (midline dimple/tuft of hair, etc.). Sacrococcygeal teratoma presents as a mid-line sacral tumor over spine at birth.
• Limbs abnormalities may be due to fetal posture, birth injury or congenital malformations. Sole creases are present up to anterior 2/3rd or more of sole in fullterms.
Common limb problems include—(a) congenital defects, e.g. poly/syndactyly, hip dislocation, clubfoot, amniotic bands, etc., (b) traumatic lesions, e.g. fractures or brachial plexus injuries. Abnormal dermatoglyphics, e.g. simian crease, may indicate chromosomal defects. All newborns, specially with breech delivery or oligohydramnios, must be screened for congenital dislocation of hip by Ortolani/Barlow test (Ch 23.2.2).
• External genitals must be examined to assess gestation and exclude ambiguous genitalia.
Afullterm male newborn has stretched penile length of 3-4 cm, less-retractile prepuce (physiological phimosis), pigmented scrotum with extensive rugae, and well-descended testes. Penile erection is common.
Important male genital problems are—micropenis (lt;2.5 cm at birth); epi/hypospadias; hyperpigmented scrotum in congenital adrenal hyperplasia; undescended testes, hydrocele and inguinal hernia. Testicular volume is unusually small in Noonan syndrome and Klinefelter syndrome and unusually large in Fragile-X syndrome.
Term female newborns have well-developed labia majora that cover gt; 2#8725;3rd of minora. A non-purulent discharge is common during 2-7th day due to transplacentally transferred maternal hormones. Some babies develop transient vaginal bleeding on 5-7th day, due to estrogen-withdrawal.
Common and usually benign female genital abnormalities include labial adhesions, imperforate hymen, hymenal tags and clitoral hypertrophy, though last may be a sign of adrenogenital syndrome. Urine is passed with 24 hours by gt;95% newborns, else should alert about possibility of obstructive uropathy, e.g. posterior urethral valves in males or dehydration.
• Anus examination is essential in cases who have not passed meconium for 48 hours and includes visual inspection. Also look for fistulous outlets.
V. Umbilical examination is an essential part of neonatal assessment, being the commonest portal of entry for infections.
Normal umbilical cord is ~30-50 cm in length and contains two arteries, one vein, remnants of omphalomesenteric (vitalline) duct, rudimentary allantois and a gelatinous substance (Wharton's jelly), all covered by amniotic sheath. Post-delivery, the umbilical stump dries-up and shrivels within 24 hours to turn yellowish black and fall-off by 7-8th day. Umbilical arteries constrict at birth or within 4-6 hours, while vein may be cannulated till 5-7th day. Later, umbilical arteries and vein form lateral umbilical ligaments and ligamentum teres, respectively.
Common umbilical anomalies at birth include:
• Single umbilical artery is present in 5-10/1000 singleton and 35-70/1000 of twin births and signifies presence of other congenital anomalies in ~ 1/3rd cases.
• Delayed separation of cord stump beyond gt;10th day indicates umbilical sepsis or defects of phagocytic function; while early separation is usually traumatic (avulsion injury).
• Umbilical bleeding may be due to—(a) slipped ligature, (b) trauma, (c) sepsis, or (d) systemic bleeding disorders.
Umbilical discharge is usually due to—(a) sepsis (purulent); but rarely may indicate, (b) patent omphalointestinal duct (fecal discharge), or (c) patent urachus (urinary discharge).
Omphalocele, i.e. herniation of abdominal contents through umbilical ring, covered only by peritoneum without overlying skin (d/d umbilical hernia) may be an isolated defect or seen in Trisomy 13 or Beckwith's syndrome. As the herniated sac may contain vital structures, e.g. intestines or liver, it should be immediately covered with sterile saline gauze to prevent drying, till surgery is arranged.
Umbilical sepsis, see Ch12.15.1.
VI. Abdominal examination includes inspection for abnormal appearance or distension (record girth, if distended) as well as palpation for liver, spleen, kidney or unusual mass. At birth, liver may be palpable up to 2 cm, as also the splenic tip and lower poles of kidneys.
Common abnormalities in appearance include:
(a) scaphoid abdomen in congenital diaphragmatic hernia, (b) distended abdomen in necrotizing enterocolitis, intestinal, obstruction or paralytic ileus, and (c) parietal wall defects, e.g. omphalocele, ectopia vesicae, gastroschisis, or prune-belly syndrome
Hepatosplenomegaly at birth usually indicates intrauterine infection. Ascites in newborns indicates: (i) hydrops fetalis, (ii) lymphatic malformations, or (iii) severe renal disease.
VII. Respiratory examination aims to assess the presence, severity and etiology of respiratory distress (Ch 12.13). Auscultatory findings are unreliable in newborns and should be supported by X-ray, if necessary.
Excessive oral frothing or gurgling sounds on chest auscultation, are warning signs for tracheo-esophageal fistula and diaphragmatic hernia, respectively.
VIII. Cardiovascular examination aims to assess: (a) location of heart sounds, as well as (b) presence of murmurs.
Presence of better audible heart sounds in right hemithorax indicate dextrocardia, situs inversus or dextroversion (due to right lung aplasia or left pneumothorax). In newborns, splitting of S2 is easily audible with loud P2 due to high pulmonary vascular resistance.
Presence of a murmur in newborn not necessarily indicates congenital heart disease, since transient functional murmurs are present in 15-20%. Conversely, the absence of murmurs does not exclude a heart disease, as many lesions manifest later when pulmonary vascular resistance drops after lung expansion.
IX. Neurological examination on first day includes assessment of—(a) general behavior, e.g. alertness, activity and cry, (b) active/passive tone, (c) symmetry of limb movements, and (d) primitive neonatal reflexes. Newborn should be neurological examined only when quiet but alert—Prechtl stage III (Table 12.11), usually after 1 hour of feeds.
• Abnormal behavior, e.g. staring spells, vacant look or shrill cry may indicate seizure activity in newborns,
TABLE 12.11: Prechtl stages of neonatal behavior
Stage Behavior
I Quiet non-REM sleep, regular breathing
II REM sleep, irregular breathing
III Quiet awake: Eyes open, minor movements
IV Active, alert, moderate movements
V Crying
REM: Rapid eye movement while sluggish activity is a warning sign for septicemia, hypothermia, hypoglycemia and asphyxia. Jitteriness indicates hypoglycemia or hypoxic brain injury.
• Tone may be assessed indirectly by posture (flexed/ extended) or directly by various methods for active tone (arm recoil) /passive tone (Popliteal angle, scarf sign, Heel-to-ear maneuvers ) (Ch 12.10.1). Hypotonia at birth is a sign of prematurity, neuromuscular disorders, birth asphyxia or critical illnesses, while Hypertonia indicates kernicterus, tetanus neonatorum or cerebral damage.
• Asymmetric limb movements may be due to true weakness, e.g. brachial plexus injury, neural tube defects, etc. or pseudo-paralysis in local painful conditions, e.g. fractures, septic arthritis, congenital syphilis, etc.
• Primitive neonatal reflexes (NNR) are excellent indicators of neurological disease (see below). Absent or sluggish NNRs usually indicate prematurity, critically sick newborn or sedation.
• Deep tendon reflexes may be exaggerated in newborns due to immature myelination and ankle clonus is common. Asymmetry of these reflexes is more informative, suggestive of neuromuscular disorders.
• Plantar response is normally extensor in newborns, with a little clinical significance.
Primitive neonatal reflexes, which appear and disappear in fairly consistent sequence during specific periods of development (Table 12.12, Fig. 12.5) are excellent indicators of neonatal health, neurological status and development. Note that:
• While most NNRs start developing in late gestation, they mature gradually to reach the optimal level only in full terms. Hence, the strength of reflex response is as important as its presence.
• Absent/sluggish NNRs, apart from illness, may also be due to physiological factors, e.g. feeding or sleep.
• Disappearance of a NNR is necessary before reaching the corresponding milestone, e.g. tonic neck reflex disappears before crawling.
• Persistence of NNRs, beyond the expected age is an important indicator of cerebral palsy.
TABLE 12.12: Common primitive neonatal reflexes
| NNR | Appears | Disappears |
| Moro's* | 28-32 weeks | 3-4 months |
| Sucking/rooting | 32-36 weeks | 4-6 months |
| Palmar grasp | 28-32 weeks | 3-4 months |
| Plantar grasp | 32-36 weeks | 8-10 months |
| Stepping | 32-36 weeks | 3-4 months |
| Crossed extension | 32-36 weeks | 4-6 months |
| Landau | 32-36 weeks | 24 months |
| Tonic neck reflex | 1-2 months | 4-6 months |
| Parachute | 6-8 months | Persists |
*Moro's is the first reflex to appear and disappear

Fig. 12.5: Common primitive neonatal reflexes.
Common primitive NNRs are as follows:
Sucking reflex is elicited by touching the baby's lips with a clean finger, leading to sucking movements that should be assessed for strength and rhythm. It is present but weak at 28th week but strong enough by 32 weeks.
Rooting reflex is elicited by stimulating the baby's lips or corner of mouth by examiner's finger, leading to movement of lips/tongue and turning of the head towards the same side, as in search of breast. Sucking and rooting reflexes together are also called cardinal point reflexes.
Moro's reflex is elicited by pulling the supine baby halfway to sitting position and suddenly letting his head fall back a short way, supported by examiner's hand. The response consists of sudden abduction and extension of arms with opening of fists (Phase I), followed by adduction and flexion in arms-embracing position (Phase II). Asymmetric Moro's reflex indicates brachial plexus injury or fracture of clavicle.
Startle reflex, elicited by sudden noise (clapping of hands) is similar to Moro's reflex, except flexion rather than extension of arms and absence of second component. Sluggish startle response indicates hearing impairment. Palmar grasp reflex is elicited by stroking the baby's palm with examiner 's index finger, leading to flexion of fingers to grasp it, which is reinforced on attempts to remove the finger. In fullterms, grasp may be strong enough to support the baby's weight. Grasp reflex has to disappear, before the baby learns to release the objects. Persistent grasp is a reliable indicator of cerebral palsy. Plantar grasp reflex is elicited by stroking the anterior 1#8725;3rd of sole, leading to flexion of toes. Plantar grasp disappears before baby learns to walk.
Stepping reflex (limb-placement reflex) is elicited by rubbing the shin of tibia on the side of table that leads to lifting of leg over table's edge.
Walking reflex is elicited by holding the baby upright and pressing the sole of one foot on couch, leading to flexion of opposite leg, as in walking.
Asymmetrical tonic neck reflex (ATNR) is elicited by turning the baby's head to one side, leading to extension of ipsilateral arm and flexion of contralateral knee (Fencer's position). ATNR has to disappear before the baby learns to turn from supine to prone position.
Symmetric tonic neck reflex is characterized by extension of arms and flexion of knees when the head is flexed and vice versa. This reflex has to disappear before the baby starts crawling.
Crossed-extension reflex is elicited by gently stroking the sole of a leg held in extension, leading to rapid flexion, adduction and then extension of opposite leg. Although this reflex appears at 32 weeks, adduction component is absent in preterms.
Parachute reflex is a protective reflex that appears before walking starts, elicited by holding the baby in ventral suspension and suddenly dropping to some distance, leading to extension of arms, hands and fingers. It is absent or asymmetric in cerebral palsy.
Landau reflex is elicited by holding the baby in ventral suspension, leading to extension of head, spine and legs. Flexion of head in this position leads to flexion of limbs.
III. Subsequent Examinations Till Discharge
Neonatal examination is never complete in one sitting. During hospital stay, all babies need to be re-examined at least twice a day for any warning sign (see Table 12.14). However, baby must not be handled too frequently to avoid infections. Routine evaluation on ward rounds include:
• History regarding—(a) acceptance of feeds, (b) passage of meconium/urine, and (c) other significant events. Failure to pass urine till 24 hours and meconium till 48 hours indicates need of detailed evaluation.
• General examination specially for—(a) behavior, activity and cry, (b) vital parameters, (c) weight record, (d) icterus, (e) umbilical sepsis, (e) superficial infections, e.g. thrush, conjunctivitis, pyoderma, rash, etc., and (g) warning/danger signs.
• Systemic examination specially for—(a) abdominal distension, (b) new murmurs, and (c) NNRs.
• Maternal examination for—(a) general health and diet, (b) local breast/nipple problems, and (c) counseling regarding breastfeeding, temperature control and good baby care practices.
IV. Examination at Discharge
A normal newborn may be discharged after 48 hours, though preterms/small for date and sick newborns need to stay longer. Examination at the time of discharge aims to ensure eventless course at home and includes:
• Thorough clinical examination to exclude danger signals and hitherto missed congenital anomalies.
• Proper maternal counseling about feeding, thermocare, immunization, follow-up, birth registration, and further family planning.
12.4
More on the topic NEONATAL RESUSCITATION:
- Chapter 10 Immediate Care of the Newborn
- Basic principles of newborn care
- Objectives and Implementation
- Transient Neonatal Myasthenia
- Transport of the Pregnant Patient
- INDIA NEWBORN ACTION PLAN (INAP)
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Perimortem Cesarean Delivery
- Decision on level of intervention
- Conjoined Twinning