Evaluation of the Patient
Careful examination of the TM in the dog or cat with otitis media requires general anesthesia. It is recommended that the patient have an endotracheal tube placed in case there is a ruptured eardrum.
Manipulation or flushing can cause material to drain through the eustachian tube into the nasopharynx, resulting in aspiration.If there is significant stenosis of the external ear canal, either from inflammation or from permanent pathologic changes to the ear canal, the eardrum may not be adequately visualized. Patient preparation using potent topical and/or systemic corticosteroids (prednisone, 1 mg/lb daily for 10 to 14 days, then taper or dexamethasone

Figure 14-5
Pharyngeal drainage of mucus from a 12-year-old cat with mucoid otitis media. The mucus drainage is coming from under the soft palate. No organisms were cultured from this cat's middle ear, but both bullae were sclerotic.
2 mg/ml at a dose of 0.1 mg/lb intramuscularly [IM] once) may be needed to reduce otic inflammation and allow examination of the TM on a subsequent visit. If permanent changes to the ear canal prevent visual determination of the integrity of the eardrum, other techniques are used to identify disease proximal to the stenosis.
Recently, with the introduction of video otoscopes, it is possible to get a very detailed, magnified examination of the ear canal and eardrum. The video otoscope provides excellent lighting at the tip of the tapered probe by transmitting light through the probe by a fiberoptic cable attached to a high-output light source.
After the veterinarian is comfortable looking at normal eardrums—the location, color, clarity, and the normal tension on it—using the TM to diagnose otitis media becomes much easier. If the eardrum remains translucent, the middle ear can be transilluminated with the bright light from the video otoscope and the contents of the middle ear can be visualized (Figure 14-6).
In obvious cases of canine otitis media, there is no eardrum present. The ear canal is filled with a liquid secretion, often with flecks of material mixed with it. A mucus- filled ear canal may alert the clinician to otitis media. Most patients with chronic otitis externa that has been present for 45 to 60 days will have a coexisting otitis media. In otitis externa, purulent exudates and proteolytic enzymes elaborated by inflammatory cells have a caustic effect on the thin epithelium of the eardrum, causing it to become necrotic, weaken, and eventually rupture. When this happens, hairs,
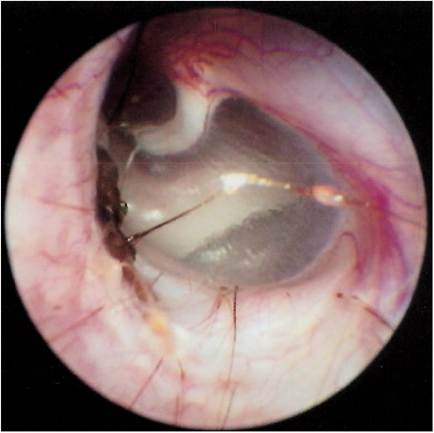
Figure 14-6
Transillumination of the TM with high-intensity light allows examination of the middle ear. Air fills the normal middle ear, and a bony prominence called the promontory (behind which is the cochlea) can be seen on the medial wall of the bulla.
ceruminous secretions, exudates, and infectious bacteria or yeast organisms in the external ear move into the middle ear. In these patients it is difficult to visualize any part of the eardrum, since it may not be present at all. Sometimes only a small ring of granulation tissue may be seen at the annulus fibrosus, where the eardrum attaches to the ear canal. With the otoscope, an otitis media case without suppuration looks like a deep, dark hole. The mucosa becomes dark as it becomes hyperemic, and brownish ceruminous exudates fill the bulla.
There is a condition described in dogs called a “false middle ear.” Obstructions along the horizontal ear canal from hypertrophic or cystic glands, neoplasia, inflammation, or ceruminous plugs increase pressure on the TM, causing it to stretch and bulge into the middle ear cavity. Coupled with poor air movement through the eustachian tube, negative pressure inside the bulla pulls the eardrum even farther into the middle ear cavity. A false middle ear may develop as a result of the distended membrane ballooning into the bulla.
Examination of this ear also reveals the absence of an eardrum at the end of the horizontal canal. Computed tomography (CT) scans of these ears reveal a “finger” lesion protruding into the bulla. The invaginating eardrum may collect large amounts of debris from the external canal such as keratin, wax, and desquamated epithelial cells. The invaginated eardrum forms a cavity that needs to be flushed out thoroughly. Often misdiagnosed as having otitis media, these patients can be retrospectively diagnosed when on 2-week recheck the previously unseen eardrum is back in the normal location.
Figure 14-7
The middle ear of this cat contains a fleshy mass that can be seen by transillumination.
In some cases of otitis media the eardrum is intact, but it may look abnormal. It may change color in response to inflammation on the medial side, becoming opaque and gray in color rather than pearly and translucent. Sometimes there is fluid behind the eardrum, and examination of the intact TM may indicate that it is bulging into the external ear. Purulent material in the middle ear may be seen as yellow fluid behind the eardrum. Early polyps and tumors in the middle ear may be seen as fleshy masses through the eardrum (Figure 14-7).
More on the topic Evaluation of the Patient:
- Evaluation of the Patient With Renal Disease
- Patient Evaluation Criteria
- Patient- and family-centered care (PFCC) is a philosophy of care that recognizes and respects the pivotal role of both the patient and the family in the delivery of medical care.
- Patient- and family-centered care (PFCC) is a philosophy of care that recognizes and respects the pivotal role of both the patient and the family in the delivery of medical care.
- Evaluation of a child presenting in the health care involves four key components, often referred with acronym HELP, i.e. History, Examination, Logical deduction and Plan of investigation. Present chapter outlines broad guidelines regarding history-taking, the first step in evaluation process.
- Ethical Requirements to the Patient
- Ethical Requirements to the Patient
- The Poisoned Patient
- Patient Condition for Transfer
- Patient Condition for Transfer
- Patient Transfers: Stable Versus Unstable
- Patient Transfers: Stable Versus Unstable
- General Care of the Hospitalized Patient
- Ethics of Critical Care Patient Management and Interactions
- Ethics of Critical Care Patient Management and Interactions
- Patient- and Family-Centered Care
- Patient- and Family-Centered Care
- Functional Evaluation
- Nerve Biopsy Evaluation
- Particularities of Field Paratuberculosis Vaccination Evaluation