Pathogenesis of Secondary Otitis Media
Due to the L-shaped configuration of the canine external ear canal, proteolytic enzymes within exudates produced as the result of otitis externa accumulate against the thinnest portion of the eardrum.
The resulting inflammation and enzymatic destruction lead to necrosis of the epithelium and supporting collagen, which results in thinning of the tympanic membrane, causing it to weaken.Ulceration along the ear canal can extend to the eardrum (Figure 14-9). The ulcerated tissue leaks serum, which can cause maceration and excoriation of the epithelium. The reaction is similar to a “hot spot” on the skin of the trunk of the dog. Liberation of bacterial proteases, collagenases, elastases, and lysozymes from phagocytic cells and epidermal maceration resulting from the excessive amount of serum in the ear canal disrupt the epithelial layers of the ear canal and can lead to either erosion or rupture of the eardrum.
Many cases of acute otitis media can be prevented. Special care in cleaning and attention to fluid pressure, especially with the use of bulb syringes used to flush the external ear canal, can prevent the high pressure from causing an iatrogenic rupture. Removal of exudates by careful flushing and suctioning of the ear canal eliminates the source of destructive enzymes acting on the eardrum. Specific therapy for infectious organisms based on cytology or culture results can shorten the course of the bacterial or fungal disease. Treatment of underlying skin disease such as atopy, food allergy, and hypothyroidism may remove or improve primary causes of otitis externa. Proper client education concerning the chronic nature of ear diseases increases compliance in allowing frequent rechecks to follow the progress of treatment. Recheck visits allow the veterinarian to examine the eardrum and to make changes in the treatment protocol when therapeutic response is inadequate.
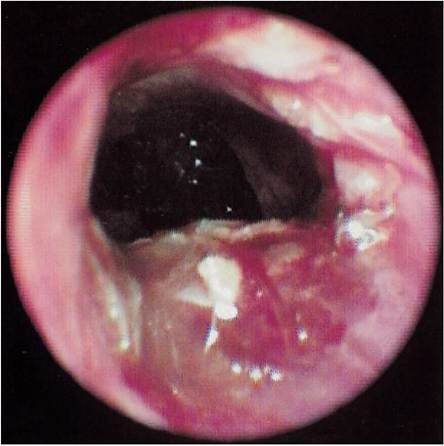
Figure 14-9
Otitis media with no eardrum present in an ulcerated ear canal. Pseudomonas was cultured from both the external ear canal and from the bulla. A slight ring of tissue (annulus fibrosus) can be seen where the eardrum was attached to the ear canal.
Whether primary or secondary, the resulting inflammation causes the lining epithelium, called the mucoperiosteum, in the bulla to change from cuboidal to pseudostratified columnar ciliated, leading to an increase in the number of secretory cells and glands, further adding to the quantity of exudate. Chronic inflammation leads to mucosal ulceration and breakdown of the epithelial lining.
The lamina propria thickens in response to inflammation, and as vascularity increases, edema and granulation tissue form. As otitis media becomes more chronic, the lamina propria changes to dense connective tissue, and bone spicules may develop within it.1
The cycle of inflammation, ulceration, infection, and granulation tissue formation may continue, destroying the surrounding bone. For example, septic arthritis of the ossicles may cause pain and decreased hearing owing to the fusion of these joints. The normal air conduction of sound waves is prevented, and the patient may suffer decreased ability to detect high-pitched sounds. With time, the ossicles are dissolved from osteomyelitis, and irreversible hearing deficit occurs.
The exudates and secretions thus formed in the bulla escape into the external ear through the ruptured eardrum and contribute to the exudate already present in the external ear canal. This large amount of liquid fills the ear canal and overflows onto the pinna when the patient shakes its head. If a polyp or tumor is blocking the outflow of secretions and exudates from the middle ear, significant quantities of inspissated material can be present when the obstruction is removed.
The fluid pressure gradient created by suppurative otitis media and increased mucus secretion prevents the eardrum from completely sealing. As the fluid pressure increases within the bulla, it pushes against a healing eardrum with a very thin, tenuous covering. The pressure allows fluid to escape through the path of least resistance, and a small hole remains in the TM. As long as there is a hole in the eardrum, this condition remains in a state of flux—that is, fluid can enter or leave the bulla, carrying infectious materials and exudates in both directions.
When the amount of middle ear secretion and exudate is decreased, when the infection is controlled by therapy, and when the fluid pressure is decreased, the eardrum can heal and otitis media resolves. Sometimes, however, the eardrum seals but the infection is not completely resolved. If the trapped organisms lead to a return of inflammation and secretion, the eardrum can once again bulge and/or rupture. Patients with otitis media may have had histories of repeated episodes because of this alternating rupture of the TM and subsequent healing. A report by Cole et al demonstrated that 70% of eardrums in documented cases of canine otitis media were intact.2
More on the topic Pathogenesis of Secondary Otitis Media:
- Secondary Otitis Media in Dogs
- Primary Otitis Media in Cats
- Otitis Media
- Treatment of Otitis Media
- Otitis media is a common disease process that often goes unrecognized in most veterinary practices.
- Microbiology of Otitis Media
- Otitis Media Prevents Healing
- The Use of Corticosteroids in Otitis Media
- 14 Diagnosis and Treatment of Otitis Media
- Net secondary production is equal to heterotroph growth
- Secondary Production
- Chronic Inflammatory Otitis
- Environmental and Conformational Causes of Ceruminous Otitis
- CONCEPT 20.4 Secondary production is generated through the consumption of organic matter by heterotrophs.
- PATHOGENESIS, PATHOLOGY AND IMMUNITY
- Energy that is derived from the consumption of organic compounds produced by other organisms is known as secondary production.
- Pathogenesis, pathology and immunity
- PATHOGENESIS, PATHOLOGY AND IMMUNITY