Treatment
Surgical Treatment
The most effective method for treating nasopharyngeal polyps is surgical because there is less chance of recurrence of the polyp. However, surgical treatment is associated with a high risk of postoperative complications.
Veterinary surgeons recommend ventral bulla osteotomy to remove the origin of the polyp as well as to culture the inflamed mucosa and institute proper antibiotic therapy.3,5 The cat has a doublechambered tympanic bulla. Exploration of the caudomedial portion, which is easily accessed through ventral bulla osteotomy, is relatively straightforward. However, exploration of the anterolateral portion requires breeching the septum that separates these two compartments. The sympathetic nerve fibers along the wall of the septum can be traumatized during this surgery. The interruption of these nerves results in Horner’s syndrome, a common postoperative sequela to ventral bulla osteotomy in the cat. After ventral bulla osteotomy, most cases of Horner’s syndrome resolve spontaneously. In addition, a branch of the facial nerve courses through the middle ear, and reversible facial neuropathy can occur as a result of trauma to this nerve. Vestibular signs such as head tilt, nystagmus, and ataxia can be associated with ventral bulla osteotomy; these signs may be irreversible.Traction/Avulsion of Polyps
Polyps can be removed from a cat’s ear canal with some type of grasping forceps through the otoscope cone. Special endoscopic tools or long alligator forceps can be used. The objective is to grasp the polyp mass and, using force, tear the attachment of the polyp away from the underlying mucosa. This is often accomplished by rotating the grasped mass 90 degrees and then applying traction. In this manner the entire polyp mass can often be removed from the mucosa lining the bulla. Increased exposure can be achieved by performing a lateral ear canal wall resection (Figure 16-6).6 Traction works best in small, non-lobulated polyps.
When removing some polyps using traction, only small pieces of the polyp can be removed. Visualization is difficult, and blood often oozes from the cut surface of the polyp mass. Repeated grasps and pulls are required to debulk the mass. This still leaves the polyp stalk in the middle ear, which may lead to regrowth of the polyp.Endoscopic Removal of Polyps
Alternative methods for dealing with nasopharyngeal polyps in the ear canals of affected cats and kittens look promising. Removal of a polyp by traction may be easier when this procedure can be viewed endoscopically using the video otoscope and endoscopic instruments. A procedure called perendoscopic trans-tympanic excision
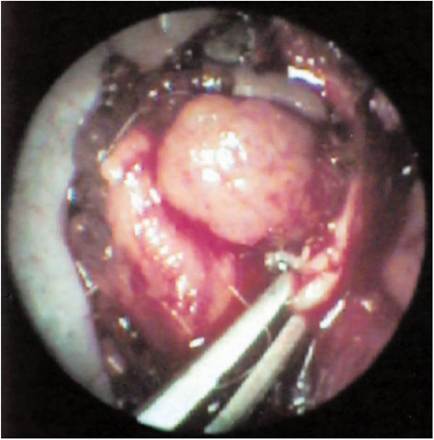
Figure 16-6
Lateral bulla osteotomy. When the polyp is inaccessible from the ear canal, an open procedure is required to excise the mass. In this cat, the polyp was not visible through the otoscope due to a stenotic condition in the vertical ear canal (a tumor) but was found during a total ear canal ablation.
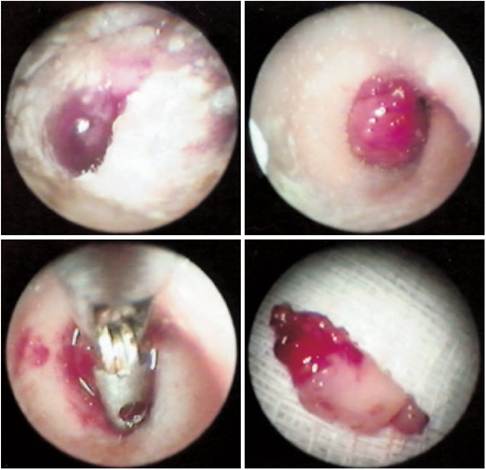
Figure 16-7
Removal of a polyp using perendoscopic trans-tympanic excision (PTTE). Top left, There is liquid in the ear canal of this cat. Top right, After cleaning, the fleshy polyp was revealed. Under direct video visualization, the polyp mass is grabbed with an endoscopic grasping forceps (bottom left) and rotated. A quick jerk on the forceps breaks the peduncle and the polyp is removed intact (bottom right).
(PTTE) has been described that uses a pinching technique with endoscopic forceps (Figure 16-7).7 The major part of the polyp can be easily removed in this manner, and the lateral portion of the bulla can be explored to remove the remnants of the peduncle. In a study of PTTE, 10 cats with polyps were treated in this manner. With follow-up endoscopic evaluations from 3 to 24 months, eight of the cats had a complete remission; only two of the cats required a second PTTE.
Two cats exhibited mild Horner’s syndrome, which was temporary.In another study of 22 cats with inflammatory polyps that were treated by traction alone, nine (41%) had recurrence. Because 59% of cats treated by traction alone had a successful outcome, these authors suggest that traction alone is a reasonable first treatment.8 Eight of the cats in this study were treated with prednisolone (1 to 2 mg/kg per day for 2 weeks, followed by half the initial dose for 1 week, and then every other day for an additional 7 to 10 days) after traction removal of the polyp. None of the cats that received prednisolone had recurrence, whereas nine of 14 cats that did not receive prednisolone had recurrences. Because it is suspected that inflammation promotes the growth of polyps, it is reasonable to assume that controlling the mucosal inflammation after removal of the polyp would retard further growth. The author routinely treats cats that have had polyps removed by traction with a combination of DMSO and a very potent corticosteroid, fluocinolone (Synotic, Fort Dodge), initially with bulla infusion through a 31/2- or 5-Fr catheter placed into the bulla and then with eardrops administered by the owners twice daily for a minimum of 3 weeks. Recurrence of the polyp is rare in these cases. In addition, azithromycin (5 mg/lb orally every other day for two or three treatments) is prescribed to treat bacterial otitis media. Cats with only nasopharyngeal polyps were nearly four times more likely to be cured by traction alone than were cats with aural polyps.
Laser Ablation of Polyps
Another promising method for aural polyp removal is laser ablation under visualization with the video otoscope. The carbon dioxide laser has been used by the author and others in the treatment of nasopharyngeal polyps. There is a special rigid laser tip, 120 mm long, that can be placed through the 2-mm working channel of one video otoscope (MedRx, Inc., Largo, Florida), so that precise laser ablation can be performed while the entire procedure is viewed on a video monitor.
Two techniques can be used in this manner.For small polyps, the laser energy is applied to the polyp mass to vaporize cells and debulk the mass. The charred tissue is removed, and the ear is flushed. This procedure is repeated for several cycles to shrink the mass and seal off the blood vessels within the polyp. The laser procedure is continued until the stalk of the polyp can no longer be visualized.
If the polyp mass is large, the 120- ? 0.8-mm tip can be extended through the 1.8-mm working channel of the endoscope into the tympanic bulla along the floor of the horizontal ear canal under the polyp mass. Laser energy is applied to vaporize portions of the polyp stalk, making traction removal easier. After the bulk of the polyp is removed from the bulla, the laser is placed into the bulla, and laser energy seals off the polyp stalk as previously described. Postoperative treatment includes the use of oral azithromycin for two or three treatments and fluocinolone/DMSO bulla infusion, followed by at-home ear drops for a minimum of 3 weeks.
Cats that have had their polyps removed rarely regrow their eardrums. Frequent reassessment of these cats is important to prevent secondary otitis media.
More on the topic Treatment:
- PRINCIPLES OF TREATMENT
- TREATMENT OF MASTITIS
- Treatment of HIV Infection
- Treatment of Otitis Media
- Treatment of HIV Pulmonary Hypertension
- TREATMENT OF INDEX CASE
- Treatment
- Treatment
- Treatment
- Treatment
- Clinical Treatment Trial for Pruritus
- STATE-OF-THE-ART HAART TREATMENT
- Assessment and Treatment of SpeechZLanguage Disorders
- Treatment of chronic adult infection