TREATMENT OF MASTITIS
The correct procedure for handling the mastitic cow was discussed on page 198. This section describes the options available for treatment.
When a milker first encounters a case of mastitis, he will have relatively little idea which organism is causing the mastitis and what the likely outcome of this particular case will be.
He has to make immediate decisions. For example, is treatment worthwhile? There is a body of opinion which says that antibiotic treatment of clinical mastitis is not worthwhile because:• Many cases are coliforms, many of which will resolve spontaneously.
• Treatment of staphylococci produces a poor bacteriological response, with only 25-40% success rate in some cases.
However, I would not subscribe to this conclusion. Whilst there is some logic in the two points above, I think that on balance antibiotic therapy is cost-effective because:
• Early treatment including first-time staphylococcal infections in heifers produces quite a good cure rate. This is shown in Tables 7.1 and 7.2. It is only older cows and long-standing infections which have such a low bacterial cure rate as 25-40%.
• Mastitis control is largely a numbers game, aimed at reducing bacterial challenge. Even if the bacteria are not totally eliminated, a reduction in their numbers should help to control spread.
• If antibiotics only contribute to saving the life of an occasional acute coliform case, they will soon pay for themselves.
Choice of Antibiotic
The choice of antibiotic for treatment should be decided after discussion with your vet, although it needs to be a broad-spectrum product, effective against staphylococci, streptococci and coliforms. He will know the type of problem on your farm and should be able to prescribe a suitable drug, although you will know the products which seem to give a better response. The technique of administering intramammary antibiotics is described on page 209.
As a general rule, streptococci are always sensitive to penicillin. However, a proportion of staphylococci (viz those which produce penicillinase) will not be, in which case the synthetic penicillins (e.g. cloxacillin) or antibiotic combinations (e.g. amoxycillin and clavulanic acid), or specific penicillinase resistant antibiotics (e.g. erythromycin, novobiocin and framycetin) will have to be used. E. coli, Pseudomonas and Klebsiella are totally resistant to penicillin, and other drugs such as the tetracyclines, cephalosporins or amoxycillin must be employed in their treatment. I think it is important to have only one, or at the most two, preparations in routine use on your farm.Taking a Milk Sample for Bacteriology
The initial choice of drug should depend on the results of a bacteriological examination of mastitis samples and the herdsman should routinely take his own milk samples for mastitis. Cleanliness is vital of course, to avoid getting false results. A good routine for milk sampling is as follows:
• Wash and dry the teat.
• Discard the first four to five squirts of milk: they may contain bacteria which have been growing in the teat canal, but which are not causing mastitis.
• Rub the end of the teat five to ten times with a swab soaked in methylated spirits.
• Only then should you open the sample bottle, keeping the lid facing downwards and the opened bottle almost horizontal. This prevents particles of dust and bacteria dropping into the bottle.
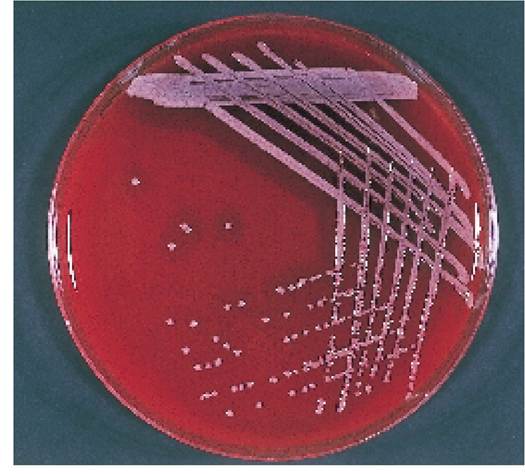
Plate 7.25. Staph. aureus growing on a blood agar plate. Each small dot in the centre of the plate is a colony, containing many millions of bacteria.
• Finally, with the bottle between the horizontal and a 45° angle, squirt in one jet of milk and replace the cover immediately.
• Label the bottle with your name, the identity of the cow, the date and the quarter sampled.
The sample should be taken to the laboratory as soon as is reasonably possible, although a delay of up to 24 hours is acceptable, provided that it is stored in a refrigerator.
At the laboratory the milk is smeared across a blood agar plate and left to grow in an incubator at 37°C for 24-48 hours. Bacteria can be seen growing as small white clumps and sometimes their appearance alone is sufficient to identify them. Plate 7.25 shows typical colonies of Staph. aureus. To confirm their identity, however, they should be stained and examined under a microscope.Antibiotic Sensitivity Testing

Plate 7.26. Antibiotic sensitivity testing. Penicillin (P 1.5) and ampicillin (PN 2) would not be effective against this strain of Staph. aureus because bacteria have grown up to the edge of the antibiotic discs.
Antibiotic sensitivity tests are performed by covering a second blood agar plate with a suspension of bacteria and then placing on small paper discs, each impregnated with a different antibiotic. After a further 24 hours incubation this second plate is examined. If the bacteria have grown up to the edge of the paper disc, then the antibiotic contained in it is not killing them. If there is a ‘zone of growth inhibition’ around the disc, however, then that antibiotic may be effective for treating the cow. Plate 7.26 shows a typical example. This strain of Staph. aureus is sensitive to all drugs tested except penicillin (P 1.5) and ampicillin (PN 2).
Factors Affecting Treatment Efficacy
There are many other factors which can affect a drug’s action, such as the ease with which the product can penetrate the udder, the concentration achieved and the persistence of the drug in mammary tissue following administration. Often the small ducts leading to the alveoli (Figure 7.1) are blocked with pus and debris and the antibiotic is simply unable to penetrate to the site of the infection. Although the clots disappear, the cow is left with a focus of infection in the udder. She is then a chronic carrier, or we may say that she has a subclinical infection.
This situation is especially common following Staph. aureus infection, although it can also occur with Strep. agalactiae and Strep. dysgalactiae.Certain strains of staphylococci and Strep. uberis may even continue to live after they have been engulfed by the neutrophils or macrophages of the udder (see Figure 7.4). Whilst inside these cells they are protected from the action of antibiotics. When the macrophage dies, however, the bacteria are released and can start multiplying again. This is another cause of the chronic carrier cow, and of mastitis which seems unresponsive to treatment. As we have already seen, subclinically affected cows are a risk to themselves in that the mastitis may recur or spread to another quarter, and they are also a danger to the other cows in the herd.
The main reasons for the poor response of Staph. aureus to treatment are:
• Many strains of Staph. aureus are resistant to penicillin and ampicillin (although all are sensitive to cloxacillin and cephalosporins).
• Staph. aureus can remain alive even when engulfed by macrophages. When inside these cells, it is protected from many antibiotics (tylosin, tilmicosin and fluoroquinolones may penetrate).
• In chronic infections, parts of the udder become walled off by fibrous tissue, so that antibiotics cannot penetrate.
• In milk, some strains of Staph. aureus become surrounded by a ‘slime’ capsule, which renders them resistant to phagocytosis.
Inserting an Intramammary Tube
Whether for the treatment of mastitis or for dry cow therapy, infusing an intramammary antibiotic is probably one of the most frequent veterinary tasks that the herdsman has to perform. Cleanliness and gentle handling are essential; otherwise infections such as E. coli or yeasts can be introduced into the udder. Only special iodine preparations (see page 220) are effective against yeasts and many dry cow tubes do not have any effect against E. coli.
If dealing with a case of mastitis, thoroughly strip out the quarter, possibly leaving it for five to ten minutes, and then strip it again.
Stripping is an excellent way of removing the bacteria and toxins. If they are not stripped out, the cow has to remove them by absorbing them into her system, and this can increase the severity of the illness. Oxytocin injections improve milk let-down.If the teats are very dirty, they should be washed and dried. Next rub the end of the teat five to ten times with a piece of cotton wool soaked in methylated spirit, alcohol or antiseptic. Only at this stage should you remove the protective cap from the nozzle of the antibiotic tube - many herdsmen find that their teeth are the best way of doing this!
Holding the teat in one hand, bend it slightly so that the orifice is pointing towards you. If the orifice is not clearly visible, draw a few drops of milk to act as a marker. Holding the tube in the other hand, gently touch the nozzle against the orifice (Plate 7.27) and then slowly slide it in. If the cow is nervous, use an anti-kick bar or get help from a second person rather than risk contaminating the tube and introducing infection. It is only necessary to insert the tip of the tube into the teat canal, as in Plate 7.27. Excess dilation of the canal can lead to cracking of its keratin lining and will predispose to mastitis. Withdraw the tube and, holding the tip of the teat between your thumb and forefinger, use the other hand to work the antibiotic up into the udder. Finally apply teat dip and then record the cow number, date of administration, quarter affected and medication used. If it was a lactating cow, make sure that she is distinctly marked so that she can be identified and her milk discarded at the next milking.
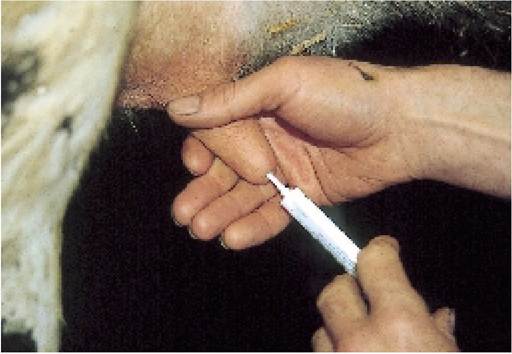
Plate 7.27. Inserting an intramammary tube. Cleanliness and gentle handling are essential.
Other Mastitis Treatments
In addition to antibiotic tubes, a wide range of other treatments has been suggested for mastitis. Antibiotics may also be given by injection and there is considerable evidence that a combined course of tubes and injections is more effective than tubes alone.
This regime is used particularly for recurrent cases and sick animals, and as the cost of antibiotics is relatively small compared with the cost of discarding milk and further cases of mastitis, many people use the combined treatments as a routine. Some antibiotics, e.g. tylosin, achieve high concentrations in the udder following intramuscular infection and have been recommended for treatment of high cell count cows.Severely ill animals need treatment for shock. This can take the form of anti-inflammatory and anti-endotoxin drugs such as flunixin and/or fluid therapy. If a cow is sick and will not drink, then fluids need to be given. The easiest way of achieving this is by mouth, for example gently running fluids from the spout of a watering can into the side of the mouth. Initial oral dosing with sodium bicarbonate may induce closure of the oesophageal groove (see Chapter 2), thereby ensuring that the fluids are delivered directly into the abomasum where absorption is likely to be better. Fluids may also be given intravenously. Intravenous hypertonic fluids, e.g. 2-3 litres of 7.2% sodium chloride, will often stimulate the cow to drink.
Continual stripping is important. This removes both bacteria and toxins and, by flushing the udder, promotes healing. Oxytocin will assist this process. If the cow has a hard, hot, swollen and painful udder she is highly unlikely to let her milk down properly. An injection of oxytocin as she enters the parlour will produce milk let-down two or three minutes later, and the milk and toxins can then be stripped from the quarter. Some people suggest the use of oxytocin alone, without additional antibiotic therapy. Whilst this may well work in a proportion of cases, it is likely that overall a better resolution of the infection will be obtained if antibiotics are administered. Topical treatments such as Cai-pan Japanese peppermint can be rubbed into the surface of the affected quarter. This probably helps the healing process by providing a massaging effect and feeling of warmth, both of which are likely to improve milk let-down and increase the feeling of well-being in the cow.
Remember that the cell count of an individual quarter stays high for at least two weeks after treatment, even if the treatment was successful at eliminating the bacteria. If possible, therefore, try to discard the milk for longer than the antibiotic withdrawal period demands, or possibly feed the milk to calves. This could be significant in reducing herd cell counts.
More on the topic TREATMENT OF MASTITIS:
- THE CONTROL OF MASTITIS
- WHAT IS MASTITIS?
- THE ENVIRONMENT AND MASTITIS
- MASTITIS RECORDS AND TARGETS
- THE MILKING ROUTINE AND MASTITIS CONTROL
- TEAT AND UDDER DEFENCES AGAINST MASTITIS
- SUMMER MASTITIS
- Mastitis continues to be a major cause of economic loss to the national dairy herd and I suspect that, combined with teat injuries, it is one of the greatest aggravations to the herdsman.
- Chapter 7 MASTITIS AND CONDITIONS OF THE TEAT AND UDDER
- PRINCIPLES OF TREATMENT
- Treatment of HIV Infection
- Treatment
- Treatment of Otitis Media
- Treatment of HIV Pulmonary Hypertension
- TREATMENT OF INDEX CASE