Myocarditis
Myocarditis is documented at autopsy in up to 50% of AIDS patients who died from noncardiac causes [2] and in 31-83% of patients with clinical signs of congestive heart failure [1].
It can be part of a disseminated infection, resulting from opportunistic microorganisms such as Candida albicans, Cryptococcus neoformans, and Toxoplasma gondii. It most often shows histological features of lymphocytic myocarditis, suggestive of a viral etiology. In fact, the presence of coxsackievirus B3, cytomegalovirus, and Epstein- Barr virus has been reported from autopsy samples from HIV-infected patients [1]. In addition, HIV-1 nucleic acid sequences have been detected by in situ hybridization in autopsy samples of patients with left ventricular dysfunction [1], most of whom had active myocarditis on histology.Pathologic Findings
On gross examination, a marked dilation of the cardiac chambers is almost always present. In most cases, owing to the focal distribution of inflammation and myocyte necrosis, the myocardium is not flabby as it is in hearts with a diffuse inflammatory response. Heart weight is within normal limits. According to the Dallas criteria [4], active myocarditis is characterized by multifocal or diffuse interstitial inflammatory infiltrates associated with degenerative changes or frank myocyte necrosis (Fig. 1). Histological findings in HIV-infected patients with myocarditis do not substantially differ from those observed in seronegative patients. However, the degree of inflammatory infiltrate is generally milder. This is believed to result from the impaired efficiency of cell-mediated immunity [2]. In addition, the inflammatory infiltrate is mainly made by CD8+ lymphocytes, and aberrant expression of class II human leukocyte antigens (HLA) by cardiac myocytes is much rarer than in HIV-negative myocarditis [5]. The severity of clinical symptoms is not always related to the degree of myocardial inflammation and damage.
Autopsy studies of AIDS patients who died of acute left ventricular dysfunction almost invariably show a marked inflammatory infiltrate [2]. However, mild and focal mononuclear infiltrates are frequently observed in hearts of AIDS patients, irrespective of the presence of cardiac symptoms.Histology and immunohistochemistry rarely detect the presence of viruses in the myocardium. However, in situ hybridization or polymerase chain reaction studies reveal a high frequency of either cytomegalovirus or HIV-1, or both, in AIDS patients with lymphocytic myocarditis and severe left ventricular dysfunction [1, 6] (Fig. 2). These data support the hypothesis that, at least in a subset of patients, HIV-1 has a pathogenic action and possibly influences the clinical evolution towards dilated cardiomyopathy [2,3].
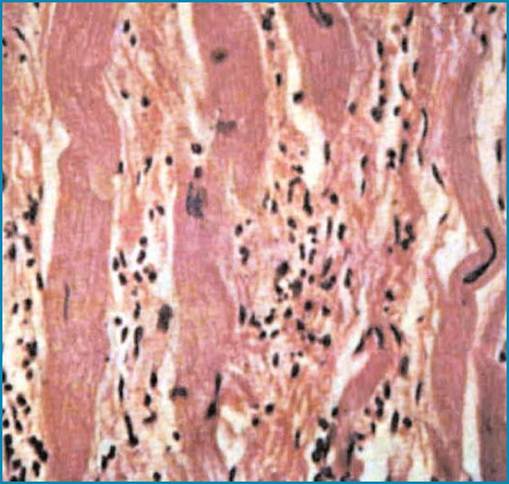
Fig. 1 AIDS-related active lymphocytic myocarditis. There is a marked interstitial lymphocytic infiltrate and myocyte necrosis. H&E, x20
Opportunistic myocardial infection is generally part of systemic infections. Fungal lesions are visible on gross examination as multiple, small, rounded plaques of whitish color, often hemorrhagic. On histology, the pathogens most frequently observed are protozoa such as T. gondii, or fungi such as Candida albicans, Cryptococcus neoformans, and Aspergillus spp. [2,3]. Myocardial and cerebral toxoplasmosis are often associated; histological examination shows “pseudocysts” packed with the protozoa within cardiac myocytes [2, 3]. Bacterial myocarditis is not infrequent in HIV-infected drug addicts with infective endocarditis. It is a consequence of coronary embolization from valve vegetations [2].
More on the topic Myocarditis:
- MYOCARDITIS
- Myocarditis
- CMR of Myocarditis
- Myocarditis
- Myocarditis or Acute Coronary Syndrome?
- Myocarditis and Viral Myocardial Infection as Causes of Cardiomyopathy
- Congestive Heart Failure
- Arrhythmias
- MYOCARDIAL DISORDERS
- Conduction System Involvement
- Conduction System Involvement
- Pathology of the Myocardium
- Pathology of the Pericardium
- Systemic Lupus Erythematosus