Rare tumours
Vaginal cancer
Role for radiotherapy by stage
Vaginal cancer represents only 3% of gynaecological cancers, and given its rarity management is based largely on single-institution experience and consensus guidelines (69).
Early stage
Stage 1 cancer limited to the vagina can often be managed by resection or partial vaginectomy with postoperative radiation or chemoradiotherapy for high-risk features such as positive margins or nodes. However, in stage 2 disease involving the paravaginal tissues or bulkier stage 1 tumours where resection may result in significant vaginal morbidity, the option for primary radiotherapy should be considered. Single-institution series have demonstrated 40-90% 5-year disease-specific survivals with radiotherapy (70, 71).
Advanced stage
Surgical treatment of advanced or node-positive vaginal cancer is limited by the extent of surgery required (total vaginectomy or exenteration) or the need for chemoradiation if nodes are positive. Chemoradiation using weekly cisplatin is increasingly considered the standard of care for both locally advanced and early disease, based in large part on the experience in cervix cancer. Limited data with chemoradiation in vaginal cancer supports this approach (72). For these reasons, chemoradiation is preferred as an organ-sparing approach.
Radiation doses and volumes are similar to those used for cervix cancer (see earlier sections), with the exception that lower-third vaginal tumours often require treatment of the inguinal nodes (similar to vulval cancer (see later sections)).
Adjuvant therapy
Adjuvant radiation/chemoradiotherapy is associated with 5-year survival rates of 69-100% in stage I/II disease (73). Neoadjuvant chemotherapy has been used prior to surgery in stage II with complete response rates of 27% (74), although similar approaches in cervical cancer are under investigation (75).
Brachytherapy
As with cervix cancer, brachytherapy plays a critical role in the management of vaginal cancers. Vaginal brachytherapy alone may be used in superficial stage I tumours with excellent results (70, 71). In stage II, the combination of external beam and brachytherapy appears to result in better outcomes (76).
Vulval cancer
Role for radiotherapy by stage
Early stage
Early-stage vulval cancer includes FIGO stages I and II (nodenegative tumours limited to the vulva with limited extension to adjacent perineal structures). The mainstay treatment for early-stage vulval cancer is surgical resection, with adjuvant radiation utilized for those patients with high-risk pathological features. Definitive radiotherapy for early-stage disease is limited to those patients who are not surgical candidates.
Advanced stage
Advanced-stage vulval cancer includes node-positive disease and/ or extensive invasion into adjacent perineal structures (FIGO stages III and IV). For those without distant metastases, radiotherapy can be delivered either as an adjuvant treatment following surgical resection or as a definitive modality. To achieve optimal results, definitive radiotherapy is often combined with chemotherapy (see ‘Definitive radiotherapy'). Radiotherapy among patients with distant metastatic disease is reserved for palliative purposes only, either to the primary or distant sites of disease.
Adjuvant versus definitive radiotherapy
Adjuvant radiotherapy
Surgical pathology of the primary site dictates the indication for adjuvant radiotherapy in the node-negative patient. Heaps et al. analysed surgical pathological variables associated with local recurrence following radical vulvectomy, revealing patients with margins less than 8 mm were at a significantly increased risk of local recurrence (77). Subsequently, Faul et al. showed that patients with close (<8 mm) or positive margins receiving adjuvant radiotherapy experienced a significant decrease in local failure, 58% versus 16% (78).
Adjuvant radiotherapy may also be considered in patients with widely clear margins if a combination of the following is present: depth of invasion greater than 9 mm, tumour thickness greater than 1 cm, lymphovascular invasion, or greater than ten mitosis per high-power field.Adjuvant radiotherapy has been shown to benefit those with multiple positive inguinal lymph nodes. GOG-37 evaluated the role of postoperative nodal irradiation in women with node-positive vulval cancer. The 6-year cause-specific survival was 71% versus 49% favouring the radiotherapy group, with an overall survival advantage being limited to patients with N2-N3 disease or with two or more positive groin nodes (79).
Definitive radiotherapy
In locally advanced vulval carcinomas, radiation has been utilized as a definitive modality, particularly when combined with chemotherapy. Support of this approach comes from two neoadjuvant trials showing a large proportion achieving complete clinical and/ or pathological response. The first GOG neoadjuvant trial evaluated split course radiochemotherapy to 47.6 Gy in patients with locally advanced T3 or T4 disease requiring an extensive resection. Following chemoradiotherapy, 46.5% had a clinical complete response and only 2.8% of patients had residual unresectable disease (80). The second GOG neoadjuvant trial used 57.6 Gy with weekly cisplatin, and 64% of patients had a complete clinical response, and 49% had a complete pathological response to combined modality treatment (81).
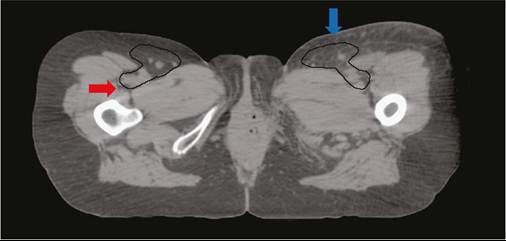
Figure 68.4 CT-based inguinal lymph node volumes. The posterior border should not extend beyond the deep margin of inguinal vessels (red arrow). The anterior border should allow for significant skin sparing, unless gross disease or skin involvement is present (blue arrow).
indicated, treatment volumes include the lower pelvic nodes and bilateral inguinal nodes.
The superior extent of coverage should include one nodal echelon cephalad to the level of clinical involvement. The caudal extent of coverage extends to cover the inguinal lymph nodes down to the saphenous vein, or lesser trochanter (82). CT- guided planning is used to assess the coverage of the lower pelvic and inguinal lymph nodes (Figure 68.4). Daily fractions are generally 1.8 Gy to a dose of 45-54 Gy in the absence of gross disease. Positive margins should be treated to 54-64 Gy, and gross disease should generally be treated to 60-66 Gy. Extracapsular extension or clinically positive lymph nodes should be boosted to 50-66 Gy depending on the volume of disease. Critical normal tissues include the femoral heads/necks, small bowel, rectum, bladder, and anus. In 3D radiotherapy, a common technique is to use a large anterior photon field in conjunction with a small posterior photon field to exclude the femurs. IMRT has been used in the treatment of vulval cancer to limit normal tissue toxicities with good outcomes (23).Ovarian cancer
Although not a rare tumour per se, ovarian cancer is now rarely treated with radiation, apart from palliative treatment to deal with recurrent inoperable symptomatic pelvic masses causing pain and bleeding.
However, there may be a role for radiotherapy in patients with rarer subtypes of ovarian cancer (clear cell and endometrioid), who tend to present with pelvic- confined disease and have lower response rates to chemotherapy. Retrospective studies show that the addition of radiotherapy to adjuvant chemotherapy (carboplatin-paclitaxel) leads to improvements in disease-free survival for patients with stage IC (cytological positivity/unknown or surface involvement) and stage II disease (83-85). The radiotherapy techniques used at that time consisted of whole abdominal-pelvic radiotherapy; however, abdominal relapses were uncommon so pelvic radiotherapy is currently used. Future clinical trials may clarify the roles of chemotherapy and radiation in these histologies (86).
Radiotherapy volumes
Treatment volumes in vulval cancer are individualized based on the clinical circumstance. The primary site, whether treated definitively or in the adjuvant setting, should include an extended margin encompassing adjacent perineal skin. When nodal radiotherapy is
More on the topic Rare tumours:
- Rare tumours
- Fallopian tube
- Vaginal cancer
- Introduction
- Origin, epidemiology, and histological classification
- Premalignant disease of the vulva
- Uterine sarcomas
- Systemic therapy in gynaecological malignancies
- Ovary
- Precision medicine-approaches to targeted therapy