Timing of Delivery in Multiple Pregnancy
Laure Noel and Basky Thilaganathan
The Facts
Importance of Dating the Pregnancy and Determining the Chorionicity
Accurate evaluation of gestational age in early pregnancy is mandatory to effect timely elective birth in both singleton and multiple pregnancies.
Recommendations on the planning of delivery in multiple pregnancies also differ based on the chorionicity. The assessment of both gestational age and chorionicity are optimally carried out by ultrasound in the first trimester.1 For in vitro fertilisation (IVF) gestations, the oocyte retrieval date or the embryonic age from fertilisation should be used to date the pregnancy.2Stillbirth Rate versus Risk of Stillbirth
Twin pregnancies are known to be at increased risk of stillbirth compared to singleton pregnancies. In a retrospective study of more than 46,000 singleton and 1,500 twin pregnancies, the stillbirth rate per fetus was fivefold higher in twin (24.8/1,000 births) compared to singleton (4.6/1,000 births) pregnancies.3 This study also demonstrated the relevance of chorionicity, as the stillbirth rates differed greatly between dichorionic-diamniotic (DCDA) and monochorionic-diamniotic (MCDA) twins at 10.8 and 58.3 per 1,000 ongoing pregnancies, respectively. However, gestation-specific by week rather than population data on stillbirth and neonatal mortality risks in multiple pregnancy are needed for clinical decisions regarding timing of birth. Here, most studies have incorrectly assumed that the stillbirth rate (fetal deaths per 1,000 total births) reflects the risk of stillbirth. Stillbirth can only occur before delivery, and therefore the risk of stillbirth is only accurately represented as a proportion of ongoing pregnancies at risk of stillbirth rather than as a stillbirth rate per 1,000 total births. When stillbirth risk is presented with the correct denominator of ongoing pregnancies, a progressive increase in this risk with advancing gestational age is evident, with this being more pronounced beyond 34 weeks of gestation (Figure 23.1).4 Due to the higher risk of stillbirth, twin pregnancies are commonly subject to physician-scheduled elective early-term birth with a worrying trend of elective preterm in monochorionic twins due to a perceived increased risk of stillbirth and subsequent demise or severe morbidity in the co-twin.
Neonatal Mortality Rate versus Risk of Neonatal Mortality
In contrast to the risk of stillbirth, the risk of neonatal complications and subsequent death decreases with advancing gestational age and increased fetal maturity. Early recommendations pertaining to timing of birth in twins only considered stillbirth risk and did not 241
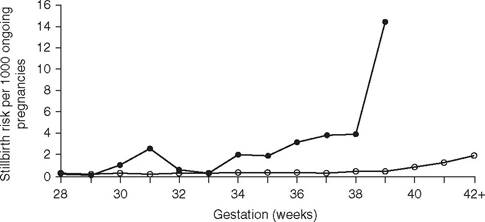
Figure 23.1 Gestation-specific risk of stillbirth per 1,000 ongoing fetuses in singletons (open circles) and twins (closed circles). Adapted from Sairam et al.4
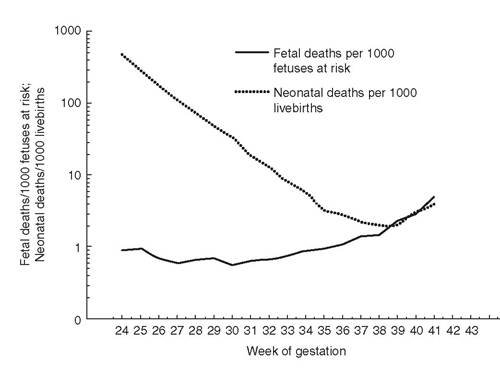
Figure 23.2 Prospective risk of stillbirth (per 1,000 ongoing gestations) and neonatal death (per 1,000 live births) in twin pregnancies. Adapted from Kahn et al.5
account for the higher risk of neonatal complications due to iatrogenic preterm or early- term birth. However, more recent data from large epidemiological datasets have compared the risk of stillbirth to the neonatal mortality rate with advancing gestation (Figure 23.2).5 Neonatal mortality can only occur after birth, so one may be excused for assuming that the neonatal mortality rate expressed per 1,000 live births accurately reflects the risk of neonatal mortality at any given gestation - in contrast to the stillbirth rate versus risk. However, neonatal mortality rate data do not account for the probability of birth at any given gestation, which differs significantly in multiple gestations compared to singleton pregnancies (Figure 23.3).6 So the accurate assessment of neonatal mortality risk needs to include the probability of birth followed by death for every week of gestation.
The Issues
Dichorionic and Monochorionic Twin Pregnancies
The optimal time for birth in uncomplicated twin pregnancies is not well established given the need to assess the prospective risk of stillbirth, the likelihood of birth and the risk of neonatal mortality for each week of gestation.
The optimal timing of delivery should be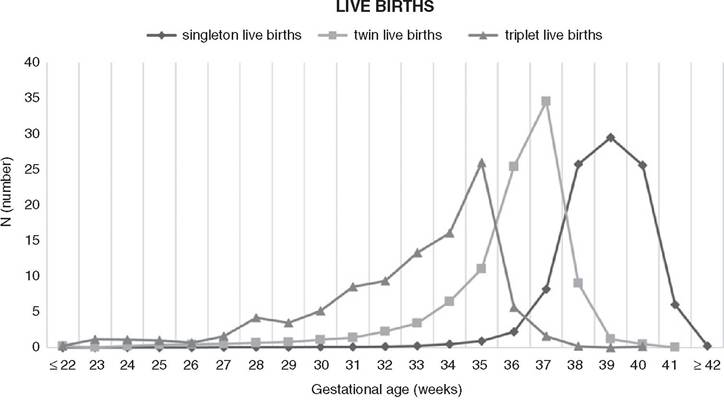
Figure 23.3 Theoveralldistributions of singleton, twin and triplet births by gestationalage. Adapted from Ko et al.6
based on the gestational age associated with the lowest risk of perinatal death. The assessment of the risk of stillbirth is complicated by the rarity of stillbirth, the need for very large population data sets, the lack of information on chorionicity, the inclusion of complicated pregnancies and the influence of antenatal monitoring protocols resulting in intervention bias. The latter have resulted in discrepancies between study findings and lack of generalisability of the data. As such, institutional and national recommendations for timing of birth vary between countries, from 37 to 39+6 weeks for DCDA twins, from 34 to 38+6 weeks for MCDA twins and from 32 to 35+6 weeks for monochorionic-monoamniotic (MOMO) twins (Table 23.1).
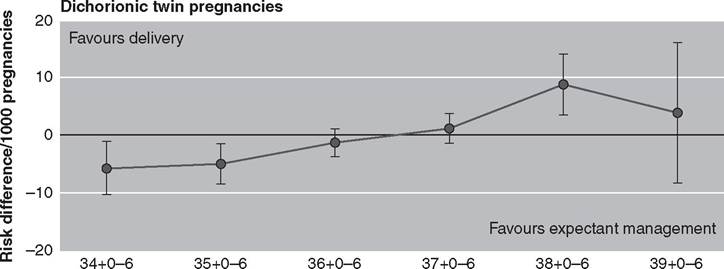
A recent individual patient data meta-analysis of 32 studies including more than 25,000 uncomplicated twin pregnancies evaluated prospective risk of stillbirth and risk of spontaneous preterm birth followed by neonatal mortality for each week beyond 34 weeks of gestation - when scheduled birth would typically be considered. The difference between risk of stillbirth and risk of neonatal death was computed to assess the benefit of expectant management versus scheduled delivery for each week of gestation (Table 23.2, Figure 23.4).7 In dichorionic twin pregnancies, the balance of risks favoured expectant management until 37 weeks of gestation. After 37 weeks, the risk of stillbirth was significantly higher than the risk of neonatal death with a risk difference above zero (Figure 23.4a). These results support the need for scheduled birth from 37 weeks in uncomplicated dichorionic twin pregnancies to optimise fetal/ neonatal outcome. In monochorionic twin pregnancies, a similar trend towards a higher risk of stillbirth was seen after 36 weeks, but this did not reach statistical significance, indicating that there is no need for elective birth before 36 weeks of gestation as has been common practice (Figure 23.4b).7
Table 23.1 Recommendations from various nationaland international guidelines for timing of birth in uncomplicated multiple pregnancies according to the number of fetuses, the chorionicity and the amnionicity
Twins Triplets
| Dichorionic- diamniotic | Monochorionic- diamniotic | Monochorionic- monoamniotic | ||
| NICE (2019) | At 37 weeks | At 36 weeks | Between 32 and 33+6 weeks | At 35 weeks* |
| ISUOG (2016) | At 37 weeks | At 36 weeks | Between 32 and 34 weeks | - |
| ACOG (2019) | At 38 weeks | Between 34 and 37+6 weeks | Between 32 and 34 weeks | - |
| RANZCOG (2017) | - | Maximum 37 weeks | - | - |
| CNGOF (2009) | Between 38 and 39+6 weeks | Between 36 and 38+6 weeks | Between 32 and 35+6 weeks | - |
| GGOLFB (2017) | Maximum 38 weeks | Maximum 36-37 weeks | Between 32 and 34 weeks | - |
For trichorionic-triamniotic or dichorionic-triamniotic triplets
NICE: NationalInstitute for Health and Care Excellence (UK); ISUOG: InternationalSociety of Ultrasound in Obstetrics and Gynecology; ACOG: American College of Obstetricians and Gynecologists; RANZCOG: Royal Australian and New Zealand College of Obstetricians and Gynecologists; SOGC: Society of Obstetricians and Gynaecologists of Canada; CNGOF: College Nationaldes Gynecologues et Obstetriciens Frangais; GGOLFB: Groupement des Gynecologues Obstetriciens de Langue Frangaise de Belgique
Monochorionic-Monoamniotic Pregnancies
The rarity of MOMO twin pregnancies has resulted in a paucity of evidence on the optimal timing of birth based on risks of stillbirth and neonatal death.
Perinatal mortality rates in MOMO pregnancies range between 10% and 40%, due to congenital anomalies, conjoined twinning, twin-reversed arterial perfusion (TRAP) sequence and large placental anastomoses predisposing to acute inter-twin transfusion.8 A previous review on perinatal outcome in MOMO twin pregnancies (n = 133) showed an overall perinatal mortality rate of 23.3% with a significant rise in perinatal deaths after 32 weeks of gestation.9 These results have been used to justify a policy of elective preterm delivery in uncomplicated MOMO twins.In a multicentre cohort study of 193 non-anomalous MOMO twin pregnancies, the prospective risk of fetal demise decreased from 16% at 11 weeks to a minimum of 1% at 28 weeks before rising to 5% at 32-34 weeks (Figure 23.5).8 However, no intrauterine fetal death was recorded in the 23 pregnancies that continued beyond 34 weeks. After 34 weeks, there was a dramatic drop in the overall risk of neonatal complications, including respiratory distress syndrome (Figure 23.5). The risks of fetal intrauterine death and non- respiratory neonatal complications were balanced at 32+4 weeks. The authors suggested that scheduled birth from 33 weeks of gestation was thus associated with the best fetal
Table 23.2 Prospective risks of stillbirth and neonataldeath per week in singleton, dichorionic and mono- chorionic twin pregnanciesfrom 34 weeks of gestation from individual patient data meta-analyses. Adapted from Muglu et al.11 and Cheong-See et al.7 Data are shown as risk per 1,000 ongoing pregnancies (stillbirths) or live births (neonataldeaths) with 95% confidence intervals in parentheses.
| Gestational age (weeks) | Singleton (n = 15,124,027) | Dichorionic twins (n = 29,685) | Monochorionic twins (n = 5,486) |
| Stillbirth risk (per 1,000 ongoing pregnancies) | |||
| 34+0-34+6 | - | 1.2 (0.7 to 1.8) | 0.9 (0.1 to 3.4) |
| 35+0-35+6 | - | 0.8 (0.4 to 1.4) | 2.8 (0.9 to 6.5) |
| 36+0-36+6 | - | 1.5 (0.9 to 2.4) | 4.5 (1.7 to 9.8) |
| 37+0-37+6 | 0.4 (0.3-0.5) | 3.4 (2.1 to 5.1) | 9.6 (3.9 to 19.7) |
| 38+0-38+6 | 0.5 (0.4-0.6) | 10.6 (7.1 to 15.3) | 7.6 (0.9 to 27.1) |
| 39+0-39+6 | 0.7 (0.6-0.8) | 9.3 (3.8 to 19.1) | - |
| 40+0-40+6 | 1.1 (0.9-1.3) | - | - |
Neonatal death risk (per 1,000 live births)
| 34+0-34+6 | - | 6.7 (3.3 to 13.5) | 12.1 (4.2 to 34.3) |
| 35+0-35+6 | - | 4.6 (2.4 to 8.7) | 8.1 (3.4 to 19.3) |
| 36+0-36+6 | - | 3.2 (1.7 to 5.9) | 5.4 (2.2 to 13.3) |
| 37+0-37+6 | 0.9 (0.5-1.7) | 2.2 (1.1 to 4.3) | 3.6 (1.2 to 11.1) |
| 38+0-38+6 | 0.4 (0.1-1.4) | 1.5 (0.7 to 3.3) | 2.4 (0.6 to 10.3) |
| 39+0-39+6 | 0.4 (0.2-0.7) | 1.1 (0.4 to 2.6) | - |
| 40+0-40+6 | 0.4 (0.2-0.7) | - | - |
outcome.
Notably, the rate of intrauterine fetal deaths was not different between women managed as inpatients or outpatients. More recently, a systematic review of 25 studies including 1,628 non-anomalous MOMO twins after 24 weeks of gestation demonstrated rates of single and double intrauterine deaths of 2.5% and 3.8%, respectively. Of intrauterine fetal deaths, 4.3% occurred before 30 weeks, 1.0% at 31-32 weeks and 2.2% at 33-34 weeks. No intrauterine fetal death was recorded from 35 weeks of gestation.10 The rates of neonatal death were 2.5% and 0.6% before 30 weeks and at 31-32 weeks, respectively, whereas no neonatal death was recorded from 32 weeks of gestation.Triplet and Higher-Order Pregnancies
Evidence for timing of delivery in triplet and higher-order pregnancies is even more scarce. The National Institute for Health and Care Excellence (NICE) in the UK recommends elective delivery at 35 weeks for trichorionic-triamniotic and dichorionic-triamniotic triplets. Individual assessment is proposed for other triplets and higher-order multiples.
Management Options
The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) published up-to-date guidance on the management of twin pregnancies in 2016.2 For uncomplicated
(a)
Gestational age (weeks)
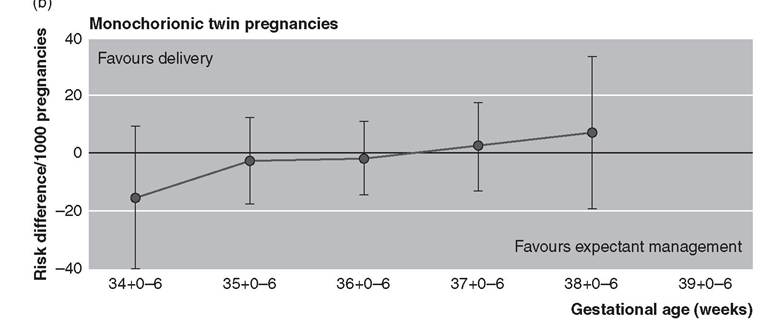
Figure 23.4 Risk difference between the prospective risk of stillbirth from expectant management and the risk of neonataldeath from delivery at weekly intervals from 34 weeks of gestation in uncomplicated dichorionic (a) and monochorionic (b) twin pregnancies. Adapted from Cheong-See et al.7
DCDA pregnancies, ultrasound assessments are recommended in the first trimester, at around 20 weeks of gestation and then every four weeks. As long as ultrasound fetal biometry, amniotic fluid volume and umbilical artery Doppler indices remain in the normal range, scheduled birth is recommended from 37 weeks of gestation.
For uncomplicated MCDA pregnancies, the ISUOG recommends ultrasound assessments in the first trimester and then every two weeks from 16 weeks onwards. At each ultrasound scan, fetal biometry, amniotic fluid volume, umbilical artery Doppler PI and middle cerebral artery peak systolic velocity should be documented. In uncomplicated MCDA pregnancies, planned delivery is recommended from 36 weeks. The management of MOMO pregnancies should take place in tertiary centres with planned delivery by caesarean section at 32-34 weeks - even though more recent evidence supports birth from 33 weeks of gestation. The antenatal surveillance strategy for uncomplicated MOMO twin pregnancies proposed by the ISUOG is similar to that of uncomplicated MCDA twin pregnancies.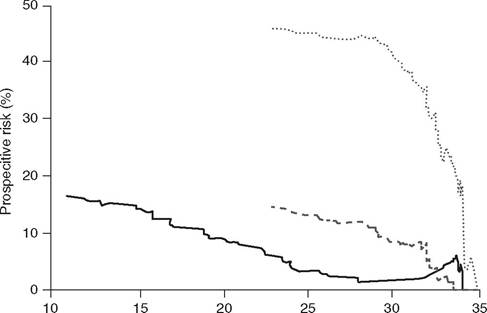
Gestational age (weeks)
Figure 23.5 Prospective risk of stillbirth and non-respiratory neonatalcomplications per gestationalage in 386 fetuses and 282 live-born neonates from monoamniotic twin pregnancies without major anomalies, respectively. Fullbold line: risk of stillbirth. Dashed green line: risk of non-respiratory neonatalcomplications. Dotted red line: risk of non-respiratory neonatalcomplications or respiratory distress syndrome. Adapted from Van Mieghem et al.8
Key Points
• An accurate evaluation of the due date and the chorionicity during the first trimester is mandatory to plan further scheduled delivery.
• Multiple pregnancies are at increased risks of neonatal deaths due to spontaneous or elective preterm delivery.
• The risk of stillbirth per ongoing pregnancies increases with advancing gestational age, whereas the risk of neonatal death per live birth decreases.
• The optimal timing of delivery should be based on the risk difference between the prospective risk of stillbirth per ongoing pregnancies and the prospective risk of neonatal death at each gestational age.
• Offer planned delivery from 37 weeks for uncomplicated DCDA twin pregnancies.
• Offer planned delivery from 36 weeks for uncomplicated MCDA twin pregnancies.
• Offer planned caesarean section at 32-34 weeks for uncomplicated MOMO twin pregnancies.
• Offer planned caesarean section from 35 weeks for uncomplicated trichorionic- triamniotic and dichorionic-triamniotic triplets.
References
1. D'Antonio F, Bhide A. Early pregnancy assessment in multiple pregnancies. Best Pract Res Clin Obstet Gynaecol 2014;28 (2):201-14.
2. Khalil A, Rodgers M, Baschat A et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol 2016;47(2):247-63.
3. Russo FM et al. Stillbirths in singletons, dichorionic and monochorionic twins: a comparison of risks and causes. Eur
J Obstet Gynecol Reprod Biol 2013;170 (1):131-6.
4. Sairam S, Costeloe K, Thilaganathan B. Prospective risk of stillbirth in multiple-gestation pregnancies: a population-based analysis. Obstet Gynecol 2002;100(4):638-41.
5. Kahn B et al. Prospective risk of fetal death in singleton, twin, and triplet gestations: implications for practice. Obstet Gynecol 2003;102(4):685-92.
6. Ko HS et al. Multiple birth rates of Korea and fetal/neonatal/infant mortality in multiple gestation. PLoS One 2018;13(8): e0202318.
7. Cheong-See F et al. Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis. BMJ 2016;354:i4353.
8. Van Mieghem T et al. Prenatal management of monoamniotic twin pregnancies. Obstet Gynecol 2014;124 (3):498-506.
9. Roque H et al. Perinatal outcomes in monoamniotic gestations. J Matern Fetal Neonatal Med 2003;13(6):414-21.
10. D'Antonio F et al. Perinatal mortality, timing of delivery and prenatal management of monoamniotic twin pregnancy: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2019;53(2):166-74.
11. Muglu J et al. Risks of stillbirth and neonatal death with advancing gestation at term:
a systematic review and meta-analysis of cohort studies of 15 million pregnancies. PLoS Med 2019;16(7)e1002838.
More on the topic Timing of Delivery in Multiple Pregnancy:
- Timing of Delivery in Multiple Pregnancy
- Antenatal care for women with a multiple pregnancy
- Planning timing and method of birth
- Practical Management of Vaginal Delivery in Multiple Pregnancy
- Multiple Pregnancy Resources for Professionals and the Public
- Management of Fetal Growth Pathology in Multiple Pregnancy
- Contents
- Maternal Complications in Multiple Pregnancy
- Mode of Delivery in Multiple Pregnancy
- Management of Monoamniotic Twins