ACID-BASE DISORDERS
Normal acid-base regulation in body revolves around the concentration of hydrogen (proton) ions in body fluids, denoted as pH-the negative algorithm of free H+ concentration.
Normal blood pH ranges between 7.35 and 7.45. H+ ions are continuously produced during various metabolic activities including dissociation of body acids (H+ donor), e.g. H2CO3 and neutralized by body bases (H+ acceptor), e.g. -OH, -HCO3, NH3, phosphates, etc.
Maintenance of normal blood pH depends on the rate of H+ ion production and their neutralization. Excess production or deficient neutralization of H+ ions lowers blood pH (acidosis), while reduced production or overneutralization leads to increased pH (alkalosis).
Thus, actual blood pH depends on a ratio between its bases and acids, also depicted by Henderson-Hasselbalch equation, i.e.
pH= pK + log base/acid
*pK is a constant, derived from dissociation of acid-base pair. As H+ ions are produced and eliminated at a variable rate, continuous regulation of normal acid-base balance depends on:
• Immediate buffering mechanisms to prevent rapid changes in pH, and
• Subsequent compensatory mechanisms to correct the actual biochemical change.
A. Buffering mechanisms: Immediately after production, H+ ions are neutralized by certain body buffers, i.e. the substances that resist sudden pH changes by accepting or releasing extra H+ ions.
The principal buffer in extracellular compartment (ECF) is bicarbonate-carbonic acid system, denoted by following bi-directional equation:
(H+) + (HCO3-) #8800; H2CO3 #8800; H2O + CO2
The direction in which this equation runs, depends on the rate of H+ production and their concentration in ECF.
From the above equation it is obvious that:• Rightward movement of this equation leads to excessive clearance of H+ ions (alkalosis), while leftward movement leads to accumulation of H+ ions (acidosis)
• Excess production of H+ or depletion of HCO3- - due to any cause, leads to excess of H+ ions in body (metabolic acidosis)
• Excess accumulation of HCO3- or depletion of H+ due to any cause, leads to deficit of H+ ions in body (metabolic alkalosis)
• Retention of CO2 due to any cause drives this equation towards left, leading to inadequate buffering of H+ ions (respiratory acidosis)
• Hyperventilation with CO2 wash-out derives this equation to the right, leading to rapid clearance of H+ ions (respiratory alkalosis)
Other important, though less efficient, buffer systems in body include, e.g. hemoglobin, proteins, phosphates, ammonia-ammonium buffer, etc.
B. Compensatory mechanisms: Abovementioned buffering mechanisms prevent rapid fluctuations in blood pH but do not correct the actual acid-base imbalance. Further, this neutralization leads to excess HCO3- utilization, disturbing normal CO2#8725;HCO3- ratio and limiting further buffering capacity.
Actual correction of acid-base imbalance after initial buffering is a slow process, which aims to normalize pCO2#8725;HCO3- ratio and eliminate excess H+ ions by:
• Pulmonary regulation, i.e. increased/decreased excretion
of CO2, by changes in respiratory rate/depth;
• Renal regulation by:
- increased/decreased reabsorption of HCO3- in proximal tubules and ascending loop of Henle,
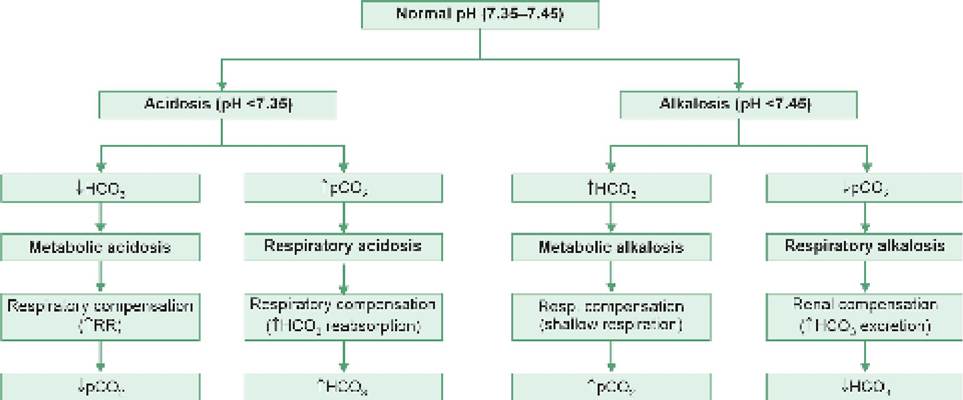
Fig. 7.4: Pathophysiology of simple acid-base disorders
- replacement of depleted HCO3- by production of new HCO3- in distal tubules and collecting ducts,
- actual H+ excretion/secretion in distal tubules and collecting ducts.
In general, metabolic acidosis or alkalosis is compensated by pulmonary mechanisms, i.e. via increased or decreased CO2 excretion respectively, while respiratory acidosis or alkalosis is compensated by renal mechanisms, i.e. increased or decreased HCO3 excretion, respectively. Thus, any acid-base imbalance is corrected by a two- step process:
a. changes due to initial buffering mechanism (primary parameter) during early stages, and
b. changes due to compensatory mechanism (secondary parameter) after some time.
As a thumb rule, in uncompensated pH disturbance, primary parameter is altered but secondary parameter is normal. On the other hand, in compensated state, primary as well as secondary parameter move in same direction. For example, in uncompensated metabolic acidosis, primary parameter (HCO3) is reduced but pCO2 is normal, while in compensated state, both HCO3 and pCO2 are reduced.
Figure 7.4 summarizes important buffering and compensatory mechanisms in various acid-base disturbances.
7.6.2
More on the topic ACID-BASE DISORDERS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Acid precipitation causes nutrient imbalances and aluminum toxicity
- EVALUATION OF ACID-BASE STATUS
- 3 Critical Care
- Cardiopulmonary Resuscitation
- Index
- Methods of intrapartum fetal monitoring
- CHRONIC KIDNEY DISEASE
- Basic principles of newborn care
- CARE OF NORMAL NEWBORN