General Physical Examination
Mukesh Agrawal
Physical examination of a young child is a skill that comes with experience. While broad principles and format of examination in children is same as in adults, following differences are noteworthy:
• The Child is usually an unwilling subject, who can disrupt the examination at any time and rarely allow the examination in an orderly sequence.
• Anxious parents present at the time of examination may interfere in the process with their own concerns, emotions and priorities.
• History is often imprecise and incomplete, making physical examination more important to arrive at a diagnosis.
• Examination needs to be modified in context of the age, in term of sequence, methodology and interpretation. It also includes additional components of anthropometry and developmental assessment. This chapter deals only with general physical examination of a child beyond the neonatal period, as examination of various systems has been discussed in respective chapters. Examination of a newborn has been discussed separately in Chapter 12.5.
General Considerations
Physical examination of children needs comfortable environment, good rapport, age-appropriate techniques and correct interpretation of findings. Some important prerequisites for good physical examination are as follows:
• Setting: Child should be examined in a comfortable and pleasant environment to ease the anxiety, with due regard to the privacy. Older or adolescent girls must be examined only in presence of a female nurse or relative.
• Rapport-building: Development of good rapport with the child is vital for successful physical examination and useful strategies include: (a) greet and introduce yourself, (b) address the child with name, (c) let the child play with examining instruments and offer some chocolate, etc., if possible, (d) allow the parents to be present and converse with them lightly while observing the child, without staring at him/her,
(e) avoid unnecessary and complete removal of cloths,
(f) explain the procedure to older children or parents,
(g) converse in a friendly manner while examining the child, to distract him/her.
• Position: Newborns, young infants (lt;3 months) and older Children (gt;3 years) can usually be examined on examination table - the best place to do so. However, older infants or toddlers are more comfortable in mother's lap or in standing position and the position of examination must be modified according to their comfort.
• Examination-kit and hygiene: All essential equipments, e.g. stethoscope, torch, measuring tape, spatula, thermometer, weighing scale and development assessment tools must be in place, in clean, working condition, to avoid unnecessary interruptions during the examination session. It is advisable to have few clean bright-color toys, which can be offered to distract the child. Examiner's hands should be washed thoroughly and warmed by rubbing against each other, before touching the child.
• Methodology: Observation is the most important step in the examination, which should begin at the level of first contact with the child and must continue throughout the history-taking and examination process. It is always preferable not to touch the young child if the desired information can be obtained by observation. Palpation must be soft and gentle, percussion to be avoided in possible and auscultation must be synchronized with respiratory phases in a crying child.
• Order and sequence: While broad protocol of examination in children is nearly same as in adults, the order of assessment must be modified according to the child's age, level of cooperation and the real need to get that information. Child is the king and examiner must try to get as much information as possible without annoying him/her. In a cardiac case, auscultation may be done prior to the palpation or percussion. Scary or painful procedures, e.g. examination of throat or reflexes must be postponed till the last, aborted at the first hint of child's discomfort. It is usually impossible to complete thorough physical examination of a child in one sitting.
• Interpretation: Examination findings in children must be interpreted in context of their age as what is abnormal in adults may be normal or physiological in young children, e.g.
jaundice in a newborn, extensor planters in infants, enlarged tonsils and lymph nodes in school-children, etc.• Documentation is essential to maintain records for future reference and legal purpose, signed and dated by examiner. All findings must be recorded as soon as possible, preferably in a pre-structured format. Figures and diagrams may be used to depict findings like rash, etc.
• Closure: At the end, examiner must discuss essential observations with the parents, but the opinion regarding diagnosis or outcome must be reserved, unless one is sure about it. It is also preferable to have light chit-chat with the child to set the stage for further interaction. Child may also be praised and rewarded with chocolate, etc. for cooperation.
Components
General examination in a child may be broadly divided into six components, as follows:
A. General appearance
B. Vital signs
C. General markers of the disease
D. Anthropometry
E. Head-to toe examination
F. Developmental assessment, if required.
A. General appearance not only points towards the severity of illness and urgency to manage but also assists in the differential diagnosis. However, looks can be deceptive and the reliability of this information depends on the experience of observer.
Assessment of general appearance includes assessment of: (a) built, (b) mental state, (c) posture, (d) movements, and (e) cry. Other important observations, e.g. abnormal odor (e.g. in poisonings) or sounds (e.g. stridor, wheeze, etc.) must also be recorded.
Table 31.1 provides broad terms used to describe common general appearance and their clinical interpretations. Some characteristically abnormal postures have been shown in Fig. 31.1.
B. Vital signs: Assessment of vital signs must receive the top priority in general examination in sick children, to identify the need for immediate attention (emergency triage). Important vital signs include: (a) body temperature,
(b) pulse or heart rate, (c) respiration, (d) blood pressure, and (e) capillary refill time; which should be interpreted in
TABLE 31.1: Components of general observation
Built
• Wasted........
(Malnutrition, FTT)• Obese (Nutritional, Endocrinal)
• Stunted (Chronic FTT)
Mental state
• Apathetic or Depressed...(Illness, Behavioral)
• Drowsy, Stupor, Comatose.... (Severe Illness, CNS)
• Irritable, restless, Delirious.... (Hyperpyrexia, CNS)
• Anxious and Scared.... (Rabies, child-abuse)
Posture preferred
• Squatting.... (Cyanotic CHD)
• Propped-up.... (CCF, severe ascites)
• Stooping-forward... (Asthma)
• Curled-up... (Abdominal pain)
• Lateral Decubitus... (Local pain)
• Decerebrate or Decorticate... (CNS lesion)
• Pithed-frog position...... (Floppy child)
• Scissoring.... (Cerebral palsy)
• Opistotonus.... (Tetanus)
Limb movements
• Unilaterally Restricted...... (Paralysis, pain)
• Abnormal..... (Seizures, Extrapyramidal lesions)
• Abnormal Gait (Table 18.1)
Cry
• High-pitched.... (Raised ICT, Kernicterus)
• Hoarse.... (Laryngitis, Hypothyroidism)
• Intermittent.... (Colic, Insect bite)
• Inconsolable..... (Severe pain or discomfort)
• Cat-like cry.... (Cri-do-chat syndrome)
• Goat-like Bleat..... (Infantile tremor syndrome)
FTT: Failure to thrive, ICP: Intracranial pressure.
Fig. 31.1: Common characteristic postures in disease: (A) Decerebrate posture; (B) Scissoring; (C) Opisthotonus; (D) Frog-like posture.
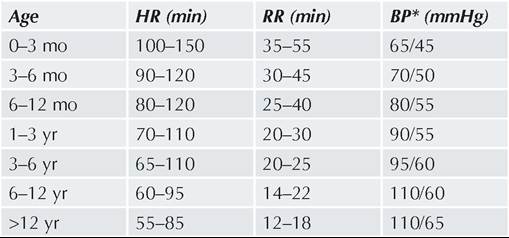
TABLE 31.2: Normal range of vital signs in children
*Lowest of the range for systolic/diastolic BP.
context of the age, considering physiological variations (Table 31.2).
Pulse must be assessed by palpation of a peripheral vessel using three-fingers—Index, middle and ring finger, for: (a) rate, (b) rhythm, (c) volume, (d) character, and (e) radio-femoral delay.
While right radial artery is usually palpated for this purpose due to ease of examination and being in direct continuation of left ventricular outflow, other vessels should also be palpated, specially - the right carotid artery for volume, femoral artery for radio-femoral delay and distal vessels, e.g.
Dorsalis pedis artery for peripheral block or thrombosis in sick children. Pulse rate must be counted for minimum one minute, though in emergency cases, pulse count for 15-30 seconds may be relied upon, multiplied by 4 or 2 respectively. In young infant, pulse may be difficult to assess and heart rate may be counted by auscultation.Pulse rate or heart rate varies with age (Table 31.2) and normal pulse is in sinus rhythm, good-bounding volume and no radio-femoral delay. For further details, see Ch 17.2.
Respiration must be observed when the child is quite and not agitated, preferably before touching the child. A young child may be observed in the mother's lap. Respiration should be assessed for: (a) rate, (b) rhythm,
(c) type, (d) work of breathing, and (e) presence of adventitious sounds.
Respiratory rate varies with age (Table 31.2). Normal respiration is regular, thoraco-abdominal (abdominothoracic in infants), effortless without use of accessory muscles and no adventitious sounds. For further details, see Ch 16.2.
Assessment of oxygen saturation by using hand-held pulse oximeter is advisable, if possible, in obviously dyspneic children. SaO2 of lt;93% in children and lt;90% in newborns indicates significant hypoxia.
Body temperature is usually recorded in oral cavity in older children and axilla or groin in younger children using mercury-free digital thermometer. Rectal temperature is rarely recorded at present and temperature
TABLE 31.3: Descriptive terms used in relation to body temperature
• Hypothermia (lt;35°C)
• Cold stress (lt;36.4°C)
• Normal (36.4-37.4°C)
• Fever (gt;38°C)
• Hyperpyrexia (gt;40°C)
recorded in ear canal by infrared thermometer or over forehead by thermo-sensitive strips, is unreliable.
Skin temperature must be recorded by cleaning the site and placing the thermometer bulb snugly at desired site and flexing the arm against the chest (Axilla) or thigh against the abdomen (Groin), for at least 2 minutes.
Oral temperature must be is recorded by placing the thermometer under the tongue and asking the child to close the mouth and breath through the nose. Oral temperature should not be recorded soon after any hot or cold drink.Oral temperature is ~0.4°C lower than rectal temperature and ~0.4°F higher than skin temperature. Temperature criteria for commonly used descriptive terms in relation to body temperature are given in Table 31.3. For further details, also see Chapters 10.1 and 12.12. Blood pressure (BP) must be recorded using appropriate cuff-size, by auscultatory method and using a mercury free sphygmomanometer, taking first and fifth Korotkoff sound as indicator of systolic (SBP) and diastolic (DBP) pressure respectively.
In infants, Flush method may be used to determine the mean BP. For further details see Ch 17.12. Normal BP varies with age as given in Table 31.2, though can also be roughly calculated as:
Normal pulse pressure (SBP-DBP) is lt;40 mm Hg. SBP is ~5-10 mm less during inspiration than in expiration. BP is also relatively higher in lower limbs (~10 mm) than in upper limbs. For further details, see Ch 17.12.
Two other important signs may also be checked at the time of recording BP in selected cases, i.e. Hess test for suspected purpura (Ch 19.10) and Trousseau sign for suspected Tetany (Ch 7.4).
Capillary refill time (CRT) indicates state of peripheral perfusion and must be checked in all sick children by pressing the thumb over a bony prominence, e.g. sternum/forehead for 5 seconds to blanch the skin. Time taken to regain the color (flush) of skin after pressure is removed denotes CRT, which should not exceed 3 seconds. Prolonged CRT indicates impending or established circulatory shock.
C. General markers of the disease: Many clinicians prefer to look for some important markers of the diseases, after the assessment of vital signs but before
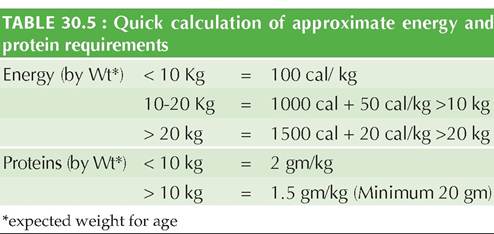
Fig. 31.2: Common clinical indicators of disease: (A) Icterus; (B) Cyanosis; (C) Clubbing; (D) Dehydration (Turgor); (E) Edema; (F) Lymphadenopathy.
exhaustive head-to-toe examination, to accelerate the process of differential diagnosis. Some important markers of disease in children include presence of: (a) pallor, (b) cyanosis, (c) clubbing, (d) icterus, (e) edema, (f) lymphadenopathy, and (g) dehydration (Fig. 31.2).
Pallor, indicative of anemia, must be assessed over palpebral conjunctiva, oral mucus membrane and palms, though severe pallor may be obvious over skin. It should not be confused with peripheral pallor due to vasoconstriction in shock or on cold exposure, which can be improved by rubbing. Pallor may be graded as Mild (limited to mucus membranes), Moderate (visible on skin/palms) and Severe (paleness of palmer creases). For further details and differential diagnosis, see Ch 19.2 and 29.1.
Cyanosis, indicative of cellular hypoxia, must be assessed over nails for peripheral cyanosis and lips/
TABLE 31.4: Grades of severity in clubbing
I. Softening of nail bed on palpation
II. Obliteration of angle at nail bed (Schamroth sign)
III. Increased horizontal or vertical curvature of nails (Parrotbeak or Drum-stick appearance)
IV. Hypertrophic osteoarthropathy (painful swelling of the hands/wrist)
tongue for central cyanosis, as bluish discoloration. Peripheral cyanosis is usually transient, due to local vascular stasis, e.g. cold or shock, and disappears rapidly on rubbing of the affected part to improve the circulation. Central cyanosis may be of pulmonary and cardiac origin, which can be further differentiated by Hyperoxia test. Cardiac cyanosis does not improve with oxygen. Differential cyanosis is limited only to either upper or lower limbs, indicative of right to left shunt at the level of patent ductus arteriosus. For further details and differential diagnosis, see Ch 17.2.
Clubbing, i.e. may be easily visible as bulbous enlargement of the nail-beds at all fingers, due to due to vascular proliferation and interstitial edema of underlying structures. However, detection of early clubbing needs palpation of the nail bed for softening or use of Schamroth sign, i.e. disappearance of the normal diamond-shaped gap, when dorsal surfaces of two opposite terminal phalanges are brought together (see Fig. 17.7). Clubbing of the toes may be normal and misleading in bare-foot walkers. Severity of the clubbing may be graded as in Table 31.4. For further details and differential diagnosis, see Ch 17.2.
Icterus, presents as yellowish discoloration of skin and mucus membranes. While it is clinically visible only when serum bilirubin levels exceed 2 mg/dl and first seen over the Sclera. More severe icterus may also be visible on the palate, undersurface of tongue and even on skin. Icterus over the sclera should not be confused with muddy sclera due to prolonged dust/smoke exposure or vitamin A deficiency. Color of the icterus may help to differentiate hemolytic (lemon-yellow) and hepatic (Golden-yellow) etiology. For further details and differential diagnosis, see Ch 15.3.
Edema denotes accumulation of excess fluid in interstitial spaces, best assessed by pressing over the suspected site for 5 seconds, leading to formation of a pit (Pitting edema). Generally, it is checked over the shins, ~2 cm above the medial malleolus. However, it must also be checked over the sacral region in young infants and bed-ridden patients, as most dependent part. The term Minimal edema is used when it can be elicited only after gt;20 seconds of pressure. Edema may be non-pitting in cases of myxedema or lymphatic obstruction. For further details and differential diagnosis see Ch 7.1.2.
Lymphadenopathy may be indicative of local or systemic pathologies, though nodes are physiologically enlarged
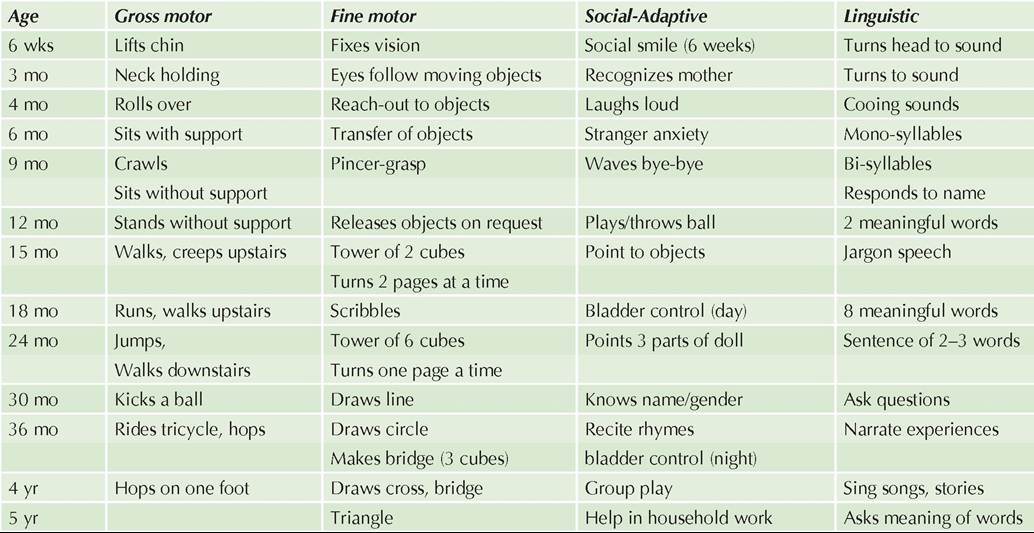
Fig. 31.3: Palpation of cervical lymph nodes: (A) From behind; (B) From front.
in early school children due to normal lymphoid growth. Examination of lymph nodes involves evaluation of various groups, e.g. cervical, axillary and femoral nodes for: (a) size, (b) location, (c) consistency, (d) tenderness,
(e) secondary changes, e.g. matting or sinus formation, and
(f) inflammatory focus in the draining area.
Cervical group is best palpated from behind with child whose neck is semi-flexed and tilted on the opposite side (Fig. 31.3). All cervical nodes, including submental, submandibular, preauricular, postauricular and occipital nodes of horizontal chain, superficial and deep cervical nodes of vertical chain, lateral cervical nodes in posterior triangle of neck and supraclavicular nodes, must be examined systematically in a sequence. Axillary nodes are best palpated by inserting the fingers in axilla with patient's arm slightly abducted. This group includes apical, anterior, posterior, medial and lateral axillary nodes. Lymph-nodes of lt;1 cm in size, discrete, mobile and non-tender are usually physiological and not significant. For further details and differential diagnosis, see Ch 19.17.
Dehydration presents with constellation of many clinical indicators, though most important examination findings include: (a) sunken eye balls, (b) depressed anterior fontanel, if open, and (c) loss of skin turgor. Skin turgor may be assessed by pinching and lifting the skin and subcutaneous tissue, usually over abdomen, for few seconds. On releasing the pinch, normal skin recoils immediately and slow or delayed recoil indicates loss of skin turgor. Assessment of turgor may be misleading in obese or severely malnourished children. For further details, see Ch 7.1.3.
D. Anthropometric parameters indicate status of growth, which can be affected by many factors, including disease. While the choice of the parameter to be recorded in a child depends on the expected problem, three basic anthropometric parameters must be recorded in all cases: (a) weight, (b) height, (c) head circumference. Additionally, mid-upper arm circumference (MUAC) must be recorded in children from 1-5 years, Body proportion parameters (Upper segment: Lower segment ratio or Arm span) in children with abnormal stature and Body mass index (BMI) in overweight children.
Anthropometric parameters recorded in an individual case must be compared with reference norms for the corresponding age and sex, using WHO growth norms/ charts (lt;5 years) or IAP growth norms/charts (gt;5 years), as discussed in Ch 2.4. Actual values beyond the ± 2 SD (lt;3rd or gt;97th percentile) of the corresponding normal values are considered as abnormal. For the sake of simplicity, actual values may also be denoted as percentage of normal values for interpretation.
For further details and methodology to record anthropometric parameters, see Ch 2.5.
Body proportions need to be assessed only in children with short or tall stature, using two parameters - Upper segment: Lower segment ratio (US:LS), also termed as CR:RH ratio (crown-to rump and rump-to heal length) and Limb span. US:LS ratio is best calculated by recording the sitting height (US) and deducting in from Standing height (LS). Limb span is recorded directly as the distance between tips of middle fingers of outstretched hands. For further details, see Ch 2.3.1.
Body mass index needs to be calculated only in apparently overweight child as weight in kg/ (Height in meter)2 For further details, see Ch 3.2.
Other anthropometric parameters, e.g. chest circumference or skin-fold thickness are of limited value in clinical practice, discussed in Ch 2.3.1.
E. Head-to-toe examination is the systematic and exhaustive evaluation of a child to search for diagnostic clues regarding the presenting illness and any coexisting health problem. Following discussion is limited to the common and important physical findings, though the actual assessment should be more exhaustive. Broadly, each organ should be examined for: (a) dysmorphic features, (b) external injury, (c) infection, and (d) medical disease, with due consideration for normal physiological variations in a growing child.
Head should be inspected for the shape, palpated over fontanels, sutures, and vault, percussed for Macewen sign and auscultated for bruit. Large head must also be tested for Transillumination. Size of the head is recorded as head circumference, discussed earlier.
On inspection, head is proportionately larger than body in infancy with mild frontal bossing. Some common abnormalities of head are shown in Fig. 31.4.
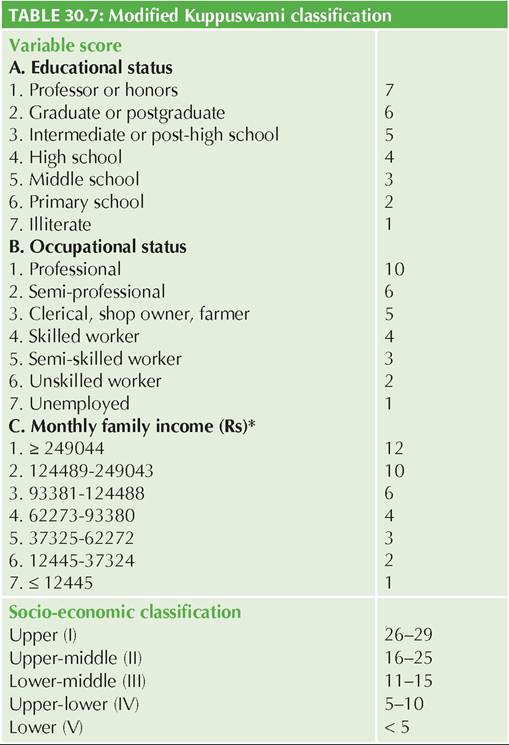
Fig. 31.4: Common head abnormalities: (A) Microcephaly; (B) Craniosynostosis; (C) Hydrocephalus; (D) Frontal bossing.
On palpation, Anterior fontanel is open (2 ? 2 cm) at birth but closes gradually over next 18 months, posterior fontanel may admit little finger at birth but definitely closes by 3 months, and sutures are palpable but not prominent. Craniotabes, i.e. Ping-pong ball like softening of skull bones felt on pressure over parietal region is normal in preterms and young infants lt; 3 months.
On percussion, Macewan sign is elicited by gentle tapping over the sutures on one side and hearing on the opposite side directly or by stethoscope (Fig. 31.5). Presence of typical crack-pot sound indicates sutural gap, seen in raised intracranial pressure. It may be normal in first 18 months, till fontanel closes.
On auscultation, cranial bruit may be normal in 15% children.
Transillumination is elicited in a dark room, by pressing the flash-light over frontal and occipital region. A rim of tranillumination exceeding gt; 2.5 cm in frontal region and gt;1 cm in other parts of scalp is abnormal.
Table 31.5 enlists important head abnormalities in children with common differential diagnosis.
Scalp must also be inspected for quantity and pigmentation of hair, infection, e.g. Lice and disease, e.g. Seborrhic dermatitis, palpated for the easy pluckability of hair and any swelling, e.g. hematoma. Distended scalp veins may indicate hydrocephalus.

Fig. 31.5: Macewan sign.
Face must be inspected for disease-specific facies (Fig. 31.6), minor dysmorphism (low-hair line, long/short philtrum), expressions, asymmetry of movements, injury, infection or disease. Mandible must be also examined for size (prognathia, retrognathia) and movements (lock jaw). Facial movements may be apparently asymmetrical in facial palsy.
Eyes must be examined for Location (hypertelorism or hypotelorism), Size (microphthalmia, proptosis), Shape (mongoloid or anti-mongoloid slant) Dysmorphism (epicanthic folds), Eyelid movements (ptosis), Extraocular movements (skew deviation, gaze palsy), Intraocular movements (nystagmus, strabismus) and other abnormal findings, e.g. injuries, infections or diseases involving lids, lacrimal system, conjunctiva, cornea, uveal tract and pupils. Lens should be examined for cataract or
31

Fig. 31.6: Characteristic facial features in common childhood diseases: (A) Down syndrome; (B) Mucopolysaccharidosis; (C) Cleft lip; (D) Cretinism; (E) Moon face (Cushing syndrome); (F) Hemolytic face; (G) Marasmus; (H) Kwashiorkor; (I) Facial palsy; (J) Adenoid facies; (K) Trismus (Tetanus); (L) Retrognathia.
cat-eye reflex followed by fundus examination in all cases with suspected neurological disorder. Careful eversion of the upper lid (Fig. 31.7) may be required in cases of suspected foreign body.
Visual acuity must be tested in all cases by age- appropriate methods (Table 26.13). Examination of color vision and field of vision is required only in selected cases. Extraocular movements must be assessed by asking to follow the examiner's instructions, though Doll's eye maneuver may be required in unconscious cases. Strabismus can be checked by Hirschberg test. Physiological squint is common in infancy. Cover test is used to differentiate paralytic from non-paralytic squint. Nystagmus, if present, must be checked for the direction.
For further details regarding common ophthalmic and visual disorders, see Ch 26. Some common ocular abnormalities are shown in Fig. 31.8.
Ears should be inspected for Location (low-set), Dysmorphism (microtia, bat-ears, pre-auricular tags) and Discharge and Palpated for tragus tenderness. Otoscopic
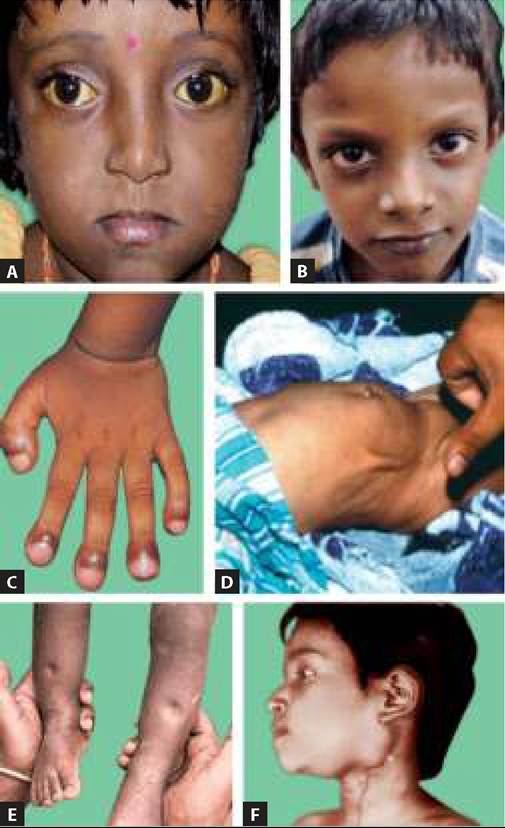
Fig. 31.7: Eversion of the lid.

Fig. 31.8: Common ocular abnormalities: (A) Proptosis; (B) Microphthalmia; (C) Cat eye reflex (Cataract); (D) Hordeolum externum.
examination is necessary in all cases with otic symptoms or hearing impairment. Low-set ears with helix below the horizontal line passing through medial canthii (Fig. 31.9), are common in many genetic disorders, e.g. Down syndrome, Turner syndrome and Di George syndrome.
Dysmorphic external ear may be associated with genetic or congenital abnormalities, e.g. microtia in goldenhar

Fig. 31.9: Important ear abnormalities: (A) Low-set ears; (B) Anotia; (C) Preauricular tag; (D) Bat ears.
or Treacher-Collin's syndrome, Bat-ears in Fragile-X syndrome, pre-auricular tags in renal anomalies and hairy-pinna in infants of diabetic mother.
Tragus tenderness, i.e. excessive cry when tragus is pressed, is a reliable sign of painful ear-canal conditions, e.g. furuncles or ear-drum inflammation, e.g. otitis media, in young infants.
Formal hearing assessment is indicated in cases with suspected deafness or delayed language development (Table 3.14).
For further details regarding common ear problems and hearing disorders, refer Ch 16.5.4 and Ch 3.8 respectively. Some common ear abnormalities are shown in Fig. 31.9.
Nose should be inspected for dysmorphic features, infection, injury, discharge and stigmata of allergic rhinitis, e.g. shiners, wrinkles or rabbit-nose. Nasal cavity must also be examined with a speculum, specially in cases with suspected foreign body, persistent nasal block/discharge (polyps, deviated nasal septum) or epistaxis. Patency of the nasal passage, e.g. in unilateral choanal atresia can be tested by spatula test.

Fig. 31.10: Common nose abnormalities: (A) Depressed nasal bridge; (B) Beak shaped nose.
Dysmorphic features may be normal or associated with other genetic or developmental anomalies, e.g. depressed nasal bridge in Down syndrome or Hurler syndrome, beaked nose in Apert syndrome or progeria, rudimentary or upturned nose in holoprosencephaly and hypoplastic alae nasi in infants of diabetic mother (Fig. 31.10). For further details regarding common nasal disorders, refer to Ch 16.5.1.
Oral cavity must be inspected externally for Dysmorphic features, e.g. cleft-lip, Symmetry during cry (facial palsy, congenital) and Lip lesions (cheilosis, angular stomatitis) and swelling of the salivary glands. Lifting of the ear pinna is an important sign of parotitis in mumps.
Oral cavity must be inspected under bright torch light for Orodental hygiene, Oral mucosa (cyanosis, dryness, Ulcers, Thrush, Koplic spots) Tongue (Color, Coating, symmetry, movements, ulcers) and Teeth (number, caries, gingival bleed/hypertrophy). Beefy red or Strawberry tongue indicates Riboflavin deficiency and Kawasaki disease, respectively.
For further details regarding common oro-dental disorders, refer to Ch 14.5. Some common oral cavity abnormalities are shown in Fig. 31.11.
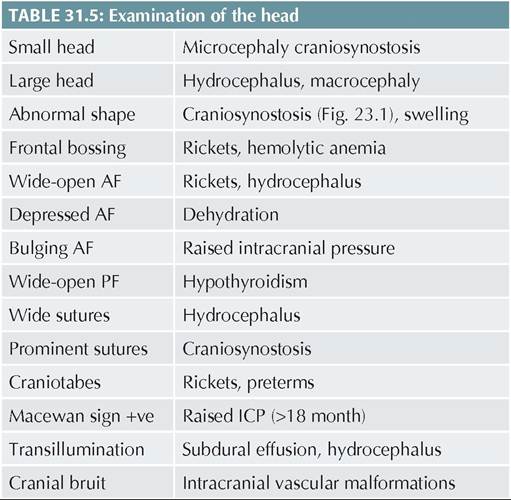
Fig. 31.11: Common oral abnormalities: (A) Cleft palate; (B) Caries; (C) Thrush; (D) Strawberry tongue.

Fig. 31.12: Diphtheria membrane.
Throat examination is often scary, and may be deferred till the end of physical examination. In an uncooperative child, it may require proper restraining in sitting or lying down position with neck extended partially with use of a spatula. Crying usually helps to see the throat, which should be examined for congestion, membranes (Fig. 31.12), tonsillar enlargement, uvular position, movement of soft palate and posterior pharyngeal wall reflex.
Throat should not examined in suspected croup till resuscitation facility is available. For further details regarding common Throat disorders, refer to Ch 16.5.2.
Neck must be examined for the length (Short, web neck in Turner syndrome, Klippel-Feil syndrome (Fig. 31.13), position (Torticolis), swelling (goiter, hygroma in midline, branchial cysts laterally), movements (neck rigidity) and prominent of veins or visible pulsations (dancing carotids).

Fig. 31.13: Neck abnormalities: (A) Webbing (Turner syndrome); (B) Klippel-Feil syndrome.
Jugular venous pressure (JVP) must be assessed in semireclining position and measured correctly (Fig. 17.6). It may be difficult to appreciate in young children, due to shorter neck and struggling child. Hepato-jugular reflux should also be checked in cases with suspected heart disease.
Skin must be inspected after proper unclothing the baby, for pigmentation, rash, bleeding, e.g. purpura, malformations, e.g. nevi, Infections and other diseases; and palpated for texture, turgor, edema and deeper lesions, e.g. nodules. Hypertrichosis may be abnormal. Evaluation of palmer creases, i.e. Dermatoglyphics, may be useful in suspected genetic disorders, e.g. Down syndrome.
Rashes must be described according to the morphology, distribution, pruritis and secondary changes (Table 25.1). Use of a magnifying glass may be necessary to confirm the subtle findings. Interdigital region must be examined carefully in case of suspected scabies. Specific signs, e.g. dermatoglyphism or Nikolsky sign must be assessed in relevant cases. Some characteristic rashes have been shown in Fig. 31.14. For further details and figures regarding common skin disorders, refer to Ch 25.
Nails must be inspected for Color (pallor, cyanosis, dyspigmentation), Deformity (platonychia, koilonychia,

Fig. 31.14: Skin rashes: (A) Macular rash; (B) Papular and pustular rash; (C) Pustule; (D) Purpuric spots.
Beau lines), infection (paronychia, onychomycosis) and palpated for clubbing and brittleness. For further details regarding common nail disorders, refer to Ch 25.11.4.
Genitals must be examined with due consideration to privacy and only in presence of a female relative in case of girls. These organs should be assessed for any morphological abnormality, e.g. ambiguous genitals, micropenis and undescended testes in males, clitoral hypertrophy in females, along with any discharge, infection or sign of sexual abuse. Some common external genital abnormalities are shown in Fig. 31.15. Sexual maturity rating (SMR) must be assessed in all school children (Table 13.2).
Back and spine must be examined for any deformity, skin lesions, swelling and tenderness. Deformities, i.e. kyphosis or scoliosis, may be congenital or acquired, e.g. Pott's spine. Presence of a non-specific skin lesion, e.g. dimple, sinus or tuft of hair must alert about the possibility of underlying neural tube defects. Bedsores are common in chronic debilitated patients. A midline swelling may be due to meningocele. Localized tenderness over spine may indicate deeper trauma or inflammatory lesions, e.g. Pott's spine. Some common Spinal abnormalities are shown in Fig. 31.16. For common Spinal problems, refer to Ch 23.2.3.
Limbs must be examined for any malformations, deformity, swelling, tenderness or restriction of movements. Any unusual or asymmetrical hypertrophy or atrophy

Fig. 31.15: Common genital abnormalities: (A) Ambiguous genitalia; (B) Clitoral hypertrophy; (C) Hypospadias; (D) Cryptorchidism.

Fig. 31.16: Spinal abnormalities: (A) Kyphosis; (B) Bed sores; (C) Sacral dimple; (D) Tuft of hair over spine.

Fig. 31.17: Common bony abnormalities: (A) Knock knee; (B) Bow legs; (C) Arthritis; (D) CTEV.
of the limb muscles may also indicate underlying neuromuscular disorders. An abnormal gait or avoi- dance/paucity of a particular limb movement may be due to neuromuscular causes (paralysis) or painful limb lesions (pseudoparalysis).
Some common orthopedic abnormalities in children are shown in Fig. 31.17. For common orthopedic limb problems, refer to Ch 23.2.2.
Bones and j oints, must be examined for any malformations, deformity, swelling, tenderness or restriction of movements. For further details regarding common orthopaedic disorders, refer to Ch 23.
Analysis of general examination: At the end of this session, physical findings must be re-arranged to:
• Correlate with history,
• Identify the system that needs to be focussed in systemic examination,
• Analyse probable differential diagnosis of the disease,
• Assess the severity of the disease process,
• Identify presence of co-pathologies,
• Plan the focus of investigations.
Analysis and interpretation of common physical findings and related information has been discussed in relevant chapters of this book.
More on the topic General Physical Examination:
- Physical Examination
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Peripheral Vascular Disease
- Basic Approach to Joint Pain
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY
- Chapter 21 Gastrointestinal, Renal, and Surgical Complications
- Bladder
- Necropsy: The Postmortem Examination
- Cases
- Inspection