PNEUMOTHORAX
Pneumothorax denotes accumulation of air within the pleural space, usually due to air-leak from underlying lung. It may also be associated with pus (pyopneumothorax) or fluids (hydropneumothorax).
Etiology: Pneumothorax may be idiopathic (spontaneous) or secondary to underlying lung disease. Staphylococcal pneumonia, congenital/acquired emphysema and iatrogenic injury due to forced mechanical ventilation are three leading causes of pneumothorax in children (Table 16.29).
Recurrent pneumothorax is seen in cases with: (a) underlying congenital cyst/bullae, (b) cystic fibrosis, and (c) collagen defects, e.g. Marfan syndrome or Ehlers- Danlos syndrome with inherently weak pleura.
TABLE 16.29: Causes of pneumothorax
• Air-leak from the lungs
- Pneumatoceles (Staph. pneumonia)
- Emphysematous bullae (asthma, foreign body)
- Congenital lung cysts or lobar emphysema*
- Cavitatory tuberculosis
- Cystic fibrosis*, #945;1 antitrypsin deficiency*
- Weak pleura* (Ehlers-Danlos syndrome)
- Iatrogenic (Forced mechanical ventilation)
• Air entry from external communication
- Trauma (penetrating thoracic injury)
- Iatrogenic (thoracocentesis/surgery)
• Spontaneous pneumotorax (idiopathic)
*Causes of recurrent pneumothorax.
Clinical manifestations depend on the amount of air collected in pleural space and generally include:
• Sudden onset or exacerbation of respiratory distress,
• Local signs—(i) bulging of chest wall on affected side, (ii) shift of mediastinum on opposite side, (iii) tympanic note on percussion, and (iv) diminished breath sounds.
• Development of severe circulatory compromise / shock indicates tension pneumothorax due to marked increase in intra-pleural pressure following continuous airleak, e.g. in bronchopleural fistula.
Diagnosis of pneumothorax should always be suspected in children with pneumonia or ventilator therapy, who develop sudden unexplained increase in respiratory distress.
Confirmation requires chest skiagram showing: (a) extreme hyperlucency with absence of lung markings, (b) underlying collapsed lung with well-defined margins, and (c) shift of mediastinum on opposite side with widening of rib spaces (Fig. 16.21). Air-fluid interface with horizontally straight level indicates hydropneumothorax (Fig. 16.22).
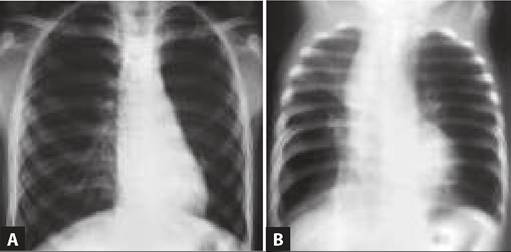
Fig. 16.21: Pneumothorax (left side).

Fig. 16.22: Hydropneumothorax (right side).
In emergency, diagnosis may be confirmed by insertion of a 21-gauze needle in 2nd intercostal space, connected to an underwater seal. Passage of air bubbles in water indicates pneumothorax.
D/D includes other causes of radiological hyperlucency, e.g. emphysema, large air-filled cavity or cysts, and diaphragmatic hernia.
Management depends on underlying cause and severity of pneumothorax and includes:
A. Removal of pleural air may be life-saving in large pneumothorax, though not necessary in all cases. General guidelines are as follows:
• Mild or even moderate size pneumothorax in an otherwise normal child, occupying lt;30% of hemithorax usually recovers spontaneously within a week. Administering 100% oxygen may hasten resolution.
• Moderate to severe pneumothorax need intercostals drainage of air (closed thoracotomy) from 2-3rd intercostal space, till the expansion of underlying lung. Two separate tubes in higher and lower intercostal spaces may be needed to drain air and pus respectively, in pyopneumothorax. Emergency needle-aspiration may be life saving in tension pneumothorax.
• Persistent or recurrent pneumothorax requires obliteration of pleural space by:
- Chemical pleurodesis, i.e. instillation of an sclerosing agent, e.g. talc, in pleural space to cause inflammatory adhesion of pleural layers, or
- Open/thoracoscopic thoracotomy with closure of bronchopleural fistula and stripping of pleura.
B. Supportive therapy includes:
• Oxygen supplementation with 100% oxygen to relieve respiratory distress and hasten absorption of air by increasing the nitrogen pressure gradient between pleura and blood.
• Treatment of primary disease, (e.g. antibiotics) and
• Symptomatic therapy for fever, pleuritic pain, etc.
Pneumomediastinum, i.e. presence of air in mediastinal space, is usually caused by rupture of alveoli in lung diseases, e.g. pneumonia or asthma: Leaked air dissects through perivascular sheaths to move toward hilum and enter the mediastinum. Air may also enter from non- pulmonary sources, e.g. esophagus following intractable vomiting, corrosive esophageal injuries/foreign bodies and chest wall trauma.
Clinical diagnosis is difficult but may be suggested by the presence of subcutaneous emphysema, obliteration of cardiac dullness or mediastinal quot;crunchquot; (Hamman sign). Final diagnosis rests on chest skiagram showing presence of air in the mediastinum.
Treatment is directed to the underlying disease and most cases resolve spontaneously. Tracheostomy or percutaneous drainage is very rarely needed to decompress the mediastinal space.
BIBLIOGRAPHY
1. Paramesh H et al. Allergic Rhinitis. Standard treatment guidelines. Indian academy of Pediatrics. 2022.
2. Chinnappa J et al. Acute otitis media. Standard treatment guidelines. Indian academy of Pediatrics. 2022.
3. Khosla et al. Sinusitis. Standard treatment guidelines. Indian Academy of Pediatrics. 2022.
4. Babu S et al. Acute pharyngitis/acute tonsillopharyngitis. Standard treatment guidelines. Indian Academy of Pediatrics. 2022.
5. Thangavelu S et al. Croup in children standard treatment guidelines. Indian Academy of Pediatrics. 2022.
6. Nanivadekar N et al. Acute epiglottitis standard treatment guidelines. Indian Academy of Pediatrics. 2022.
7. Chatterjee P et al. Bronchiolitis standard treatment guidelines. Indian Academy of Pediatrics. 2022.
8. Global strategy for asthma management and prevention (GINA) guidelines 2023.
https://ginasthma.org/wp- content/uploads/2023/07 / GINA-2023-Full-report- 23_07_06-WMS.pdf9. Roy S et al. Bronchial asthma standard treatment guidelines. Indian Academy of Pediatrics. 2022.
10. Modak S et al. Under 5 wheeze standard treatment guidelines. Indian Academy of Pediatrics. 2022.
11. Indian Academy of Paediatrics National Respiratory Chapter. Asthma training module, 2021.
12. Sukumaran TU et al. Community acquired pneumonia standard treatment guidelines. Indian Academy of Pediatrics. 2022.
13. Mathew J et al. Atypical bacterial pneumonia. Standard treatment guidelines. Indian Academy of Pediatrics. 2022.
14. Gowrishankar NC et al. Empyema. Standard treatment Guidelines. Indian Academy of Pediatrics. 2022.
15. Pacilli M et al. Management of paediatric empyema by video-assisted thoracoscopic surgery (VATS) versus chest drain with fibrinolysis: systematic review and meta-analysis. Paediatr Respir Rev. 2019;30:42.
16. Balaji S et al. Pneumothorax in children. Standard treatment guidelines. Indian Academy of Pediatrics. 2022.
More on the topic PNEUMOTHORAX:
- Pneumothorax
- LUNG ABSCESS
- CONGENITAL LUNG MALFORMATIONS
- Lymphangioleiomyomatosis
- Hemoptysis
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Cardiopulmonary Resuscitation
- Asthma
- Interstitial Lung Disease
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020