URINARY TRACT INFECTIONS
TABLE 21.26: Predisposing factors for urolithiaisis
• Metabolic causes
- Hypercalciuria
#9830; Idiopathic hypercalciuria*
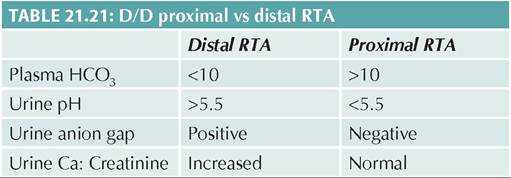
#9830; Renal tubular acidosis*
#9830; Hypercalcemic states (#8593; PTH, Vitamin D toxicity)
#9830; Others: Prolonged immobilization, steroids
- Hyperoxaluria (primary, malabsorption)
- Hyperuricemia (cytotoxic therapy, gout)
- Cystinuria (hereditary)
• Urinary tract infection
• Urinary stasis (obstructive uropathy)
• Foreign body, e.g.
prolonged catheterization• Idiopathic - Endemic vesical stones
*despite normal or low serum calcium levels
Urinary tract is the third commonest site of infection in children after gut and respiratory tract, involving lower urinary tract (cystitis) or upper urinary tract (pyelonephritis), or both.
Urinary tract infection (UTI) is defined as the growth of a significant number of microorganisms of a single species in the urine, in presence of symptoms.
Prevalence: About 1-2% boys and 3-7% girls experience at least one attack of symptomatic UTI by 6 years of age. In addition, asymptomatic bacteriuria is seen in 1-3% of infants, pre-school children and school-age girls (not boys).
While in neonatal period, UTI is more common in males (5:1) due to higher incidence of congenital urinary
tract anomalies, sex distribution equals in infancy, followed by marked female preponderance in older children/adolescence (1:10) due to shorter urethra and poor perineal hygiene.
Predisposing factors: Three most important predisposing factors for UTI are—(a) urinary stasis or obstruction, (b) ascending infection due to vesicoureteric reflux or repeated catheterization, and (c) poor perineal hygiene, e.g. pin-worm infestation or constipation (Table 21.28). Obstructive lesions are present in 10-20% of cases with recurrent UTI.
Etiopathogenesis: UIT is predominantly an ascending infection from periurethral flora, except in newborns and infants, where renal parenchyma may be directly infected during septicemia from distant sites (hematogenous spread).
Common causative pathogens for UTI include:
• Gram-ve: E. coli, Klebsiella, Proteus, Pseudomonas
• Gram +ve: Staph. epidermidis, Strept. faecalis
• Others: Candida, Adenovirus (cystitis)
Over 75% of community-acquired UTI are due to
E. coli, while nosocomial infections are usually caused by Klebsiella, Pseudomonas, Candida or Gram-positive pathogens. Proteus infection is more common in males. Clinically, UTI may present as—(a) asymptomatic bacteriuria (positive urine culture, without symptoms), (b) symptomatic lower UTI or cystitis, (c) upper UTI or pyelonephritis, or (d) chronic or recurrent UTI.
Cystitis, presents with urinary complaints, e.g. dysuria, frequency, urgency, incontinence and suprapubic pain. Fever is uncommon. Most UTIs in first 5 years of life have associated upper UTI or pyelonephritis.
Pyelonephritis, the most serious form, presents as high fever with chills, nausea/ vomiting, and abdominal flank pain. In newborns, it may also presents as septicemia, e.g.
TABLE 21.28: Predisposing factors for UTI
• Urinary stasis
- Obstructive uropathy
#9830; Congenital anomalies of urinary tract
#9830; Neurogenic bladder
#9830; Others, e.g. stones
- Voluntary urine retention in females
• Easy ascend of infection
- Short urethra in females
- Vesicoureteric redux (VUR)
- Urinary catheterization
• Altered perineal flora
- Un-circumcised males
- Constipation/encopresis
- Pin-worm infestation
- Poor hygiene, e.g. tight underwear
- Prolonged antibiotic therapy fever/hypothermia, poor feeding, diarrhea/vomiting, unexplained jaundice, shock, etc.
Chronic Or recurrent UTI may be asymptomatic or presents with failure to thrive, prolonged pyrexia and occasionally hypertension due to post-infective renal scarring, apart from recurrent attacks of acute UTI.
UTI is also classified as—(a) complicated, in presence of high fever, persistent vomiting, dehydration, systemic toxicity, renal angle tenderness or elevated creatinine values, or (b) uncomplicated or simple, in absence of these features.
Laboratory diagnosis of UTI may be divided into three stages—(a) diagnostic confirmation of UTI, (b) d/d between upper and lower UTI, and (c) identification of underlying pathology.
(a) Diagnosis of UTI rests on the presence of pus cells and bacteria in urine, followed by confirmation on urine culture (Table 21.29).
• Presumptive diagnosis can be made in presence of significant pyuria, i.e. gt;10 cells/mm3 in uncentrifuged or gt; 5 cells/hpf in centrifuged urine sample.
However, isolated pyuria without bacteriuria does not necessarily indicate UTI and may occur in any febrile illness, renal tuberculosis, interstitial nephritis or schistosomiasis. Similarly, absence of pyuria does not exclude UTI as frequent voiding in infants may not allow sufficient stay of urine in bladder to form pus cells. Pyuria may also be absent due to disintegration of cells on delayed urinalysis or poor inflammatory response in immunodeficient hosts.
Rapid Dipstick tests based on detection of nitrites or Leukocyte esterase in urine are useful screening test to detect presence of bacteria or pus cells in urine respectively. However, a positive dipstick test should always be confirmed by urine culture.
• Microbiological confirmation requires urine culture from a sample, collected by (a) suprapubic puncture (most reliable but invasive), (b) urethral catheter (specially in infants when suprapubic puncture is not possible), and (c) mid-stream clean-catch method in older toilet-trained children. Cultures from urine bags or diapers are not acceptable. Specimen should
TABLE 21.29: Diagnostic indicators for UTI
be processed within an hour of collection but may stored at 4°C up to 24 hours. Interpretation of culture reports depends on the method by which sample was collected (Table 21.29). Urine culture must be repeated in clinical suspected cases of UTI with unequivocal colony count or polymicrobial growths.
(b) Differentiation between upper and lower UTI in children is difficult in children and not essential for treatment purpose, though involvement of upper urinary tract (pyelonephritis) is indicated by presence of: (a) high fever/toxemia, (b) positive blood culture, and
(c) antibody-coated bacteria in urine.
(c) Identification of underlying pathology: Asymptomatic bacteriuria, even if persistent, does not require detailed investigations except USG, as it is often caused by persistence of low-virulence, non-invasive E. coli, without underlying anatomical/functional defect.
Further evaluation for underlying pathology is indicated in all cases of UTI, though may be deferred till second attack in older girls with simple uncomplicated UTI. Imaging studies include: (a) USG for structural malformations, VUR and renal scarring, (b) MCU for obstructive uropathy or vesicoureteric reflux, and
(c) DMSA scan to assess renal scarring and excretory function. However, the need for each investigation varies with age.
• Children lt;5 years with first attack of UTI must be screened with USG soon after the diagnosis and those with abnormal USG or recurrent non-E. coli UTI must be investigated by MCU after 2-4 weeks and DMSA after 4-6 months.
• Children gt;5 years must be screened with USG and further evaluation with MCU is needed only in those with abnormal USG and recurrent UTI. DMSA is not routinely advised in older children.
Management: No treatment is needed for asymptomatic bacteriuria except periodic urinalysis, which usually resolves in 6 months without renal scarring.
Management of symptomatic UTI may be divided into—(a) treatment of acute attacks, (b) treatment of underlying cause, and (c) prevention of recurrent attacks. Management of acute attack includes supportive therapy and specific antibiotics (Table 21.30).
Antibiotic therapy: While simple or uncomplicated UTI in children gt;3 months may be treated with oral antibiotics for 5-7 days, complicated attacks or any attack lt;3 months of age, need parenteral therapy for at least first 48-72 hours, followed by completion with oral antibiotics for total 7-10 days (10-14 days in infants).
Urine culture should be repeated after completion of treatment to exclude persistent infection. Complicated UTI, which does not respond to IV antibiotics in 48 hours, must be reassessed with USG and repeat urine culture.

Supportive therapy in UTI includes—(a) plenty of oral fluids to dilute infection, (b) frequent emptying of bladder, and (c) Symptomatic antipyretics and antispasmodics to relive pain/fever. Urine alkalinizing agents may be used to relieve dysuria, though no necessary in all cases.
Prevention of recurrent UTI: Apart from correction of predisposing factors, e.g. obstructive lesions, long-term antimicrobial prophylaxis is indicated in—(a) all children with high grade VUR, (b) all infants with any VUR, and (c) all children with recurrent febrile UTI, specially in presence of bladder-bowel dysfunction.
Single bed-time dose of oral cotrimoxazole (1-2 mg/ kg), nitrofurantoin (1-2 mg/kg) or cephalexin (10 mg/ kg) or cefadroxil (5mg/kg) may be used for prophylaxis, though first-two drugs must be avoided in infants lt; 3 months or G6PD deficiency.
Antibiotic prophylaxis must be continued in infants till 2 years of age or at least 1 year after the last attack, and in older children till resolution of VUR or bladder bowel dysfunction.
Outcome of UTI depends on presence/absence of underlying pathology and secondary renal damage before diagnosis. Each attack of UTI may accentuate renal scarring with consequent risk of hypertension and chronic renal insufficiency in later life.
Genitourinary Tract Tuberculosis
Genitourinary tuberculosis is uncommon in childhood, usually seen after more than 5 years of primary infection.
Infection is acquired hematogenously and preferentially localized at—(a) juxtamedullary region, (b) trigone/periuretetic region of bladder, (c) prostrate in males and fallopian tubes (90%) in females.
Pathologically, renal lesions may persist as asymptomatic granuloma or progress with caseation/fibrosis to cause—(a) hydronephrosis/pyonephrosis, (b) perinephric abscess, (c) renal cavity, (d) miliary lesions, or (e) ureteric deformities. Renal failure is rare.
Symptomatic cases may present with—(a) painless hematuria, or (b) recurrent UTI or pyuria without bacteri- uria, and (c) sterility.
Diagnosis rests on positive urine culture or molecular diagnosis and treatment includes specific antitubercular therapy (Ch 10.13) as per sensitivity profile, along with supportive measures.
21.16
More on the topic URINARY TRACT INFECTIONS:
- URINARY TRACT INFECTIONS
- Catheter-Associated Urinary Tract Infection
- Genitourinary Infections
- URINARY TRACT MALFORMATIONS
- Mice are susceptible to respiratory tract infections with two members of the Paramyxovirus family,
- Cystitis
- UVEAL TRACT DISORDERS
- Coccidioides Immitis Infection
- Klebsiella spp. Infection
- STREPTOCOCCAL INFECTIONS