Copper
Copper accumulation can be detected in Romanowsky-stained cytologic preparations as a blue–green to gray cytoplasmic crystalline material (Figure 9.18a). Copper content is not always readily apparent by Romanowsky staining but can be highlighted using rubeanic acid or rhodanine stains (Moore et al., 2016; Figures 9.18b, c).
Based on the low incidence of pathologically significant amounts of copper in the typical cytologic case stream, copper staining is recommended when there is a clinical concern for copper hepatopathy or an unknown pigment is found (Moore et al., 2019). Often increases in liver enzyme activity are the only sign of copper accumulation (Rodrigues et al., 2020). A copper grading system has been proposed which showed good correlation with quantitative hepatic copper content but does not allow distinction of where the copper is deposited within the hepatic lobule.Hepatic copper accumulation has been associated with chronic hepatitis and altered excretion during cholestasis in both canine and feline patients (Whittemore et al., 2012; Hurwitz et al., 2014; Cedeño et al., 2016; Eulenberg et al., 2018). Data also suggest that copper may induce chronic hepatitis and contribute to the development of hepatocellular carcinoma (Harro et al., 2019). A genetic copper hepatopathy has been demonstrated in Bedlington Terriers, Labrador Retrievers, and other dogs (Hoffmann, 2009). The amount of copper accumulated in the liver of Labrador Retrievers with primary copper hepatopathy is correlated with dietary copper content (Fieten et al., 2012). Primary copper-associated hepatopathy was seen in young cats without cholestasis, suggesting genetic or environmental causes in the cat (Hurwitz et al., 2014).
Hemosiderin/hematoidin
Hemosiderin and its iron-free homologue, hematoidin, are present in patients with increased erythrocyte turnover (hemolytic anemia or recent transfusion) and portosystemic shunts.
Hemosiderin-laden macrophages are noted with copper toxicity (Smedley et al., 2009). With Romanowsky staining, hemosiderin is a brown to blue–black coarse pigment. Hematoidin appears as orange rhomboid, refractile crystals. One relatively easy confirmation of hemosiderin presence is to observe the material within erythrophagocytic cells (Figure 9.19a). Because hemosiderin contains iron, it will stain strongly positive with the Prussian blue reaction (Figure 9.19b). Hematoidin is distinctive enough that it does not need a confirmatory stain. Since hematoidin is iron-free, hematoidin will not stain with the Prussian blue reaction. 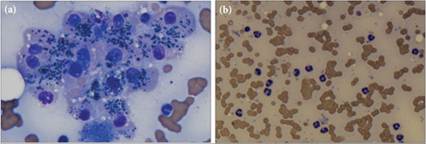
Figures 9.17a,b Canine liver sample. (a) The hepatocytes from this dog have blue to blue–green cytoplasmic material, most consistent with lipofuscin. A platelet clump is also noted in the lower center of the image (Wright–Giemsa, 1,000? magnification). (b) Neutrophils within the hepatocyte clumps, a feature commonly used to aid the diagnosis of suppurative hepatitis, are not found. The neutrophil count in this liver aspirate is higher than that of peripheral blood and myeloid precursors are not found (helping to exclude peripheral blood contamination and extramedullary hematopoiesis, respectively) (Wright–Giemsa, 500? magnification). This patient was given a diagnosis of mild suppurative hepatitis.
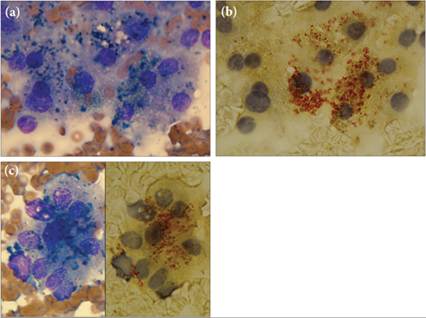
Figures 9.18a–c Seven-year-old Labrador Retriever. The patient had normal serum liver enzyme values but hypoechoic areas on ultrasound evaluation of the liver. (a) Hepatocytes with dark blue–black and pale blue–green to blue–gray cytoplasmic granules were noted (Wright–Giemsa, 1,000? magnification). (b) The blue–green to blue–gray granules stained orange–brown after rhodanine staining, consistent with copper.
Copper granules were present in only some of the hepatocytes. The darker blue–black granules likely are lipofuscin (Rhodanine, 1,000? magnification). (c) Side-by-side images of a cluster of hepatocytes with copper granules. Copper can occasionally be visually identified by Wright–Giemsa staining; however, it is more challenging to discern when amongst other pigments. Quantitative copper measurement was recommended to rule out pathologic levels of hepatic copper (left panel, Wright–Giemsa, 1,000? magnification; right panel, Rhodanine, 1,000? magnification)
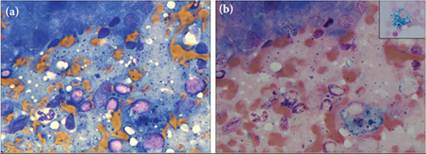
Figures 9.19a,b Nine-year-old Terrier-cross dog with a 6-month history of weight loss and recently elevated liver enzymes. (a) Clusters of hepatocytes are present in the upper left corner. There is a mixed lymphoid population with small lymphocytes predominant, suggestive of lymphocytic inflammation. The blue–black granules are suggestive of hemosiderin. A pigment-laden macrophage is present in the lower right corner (Wright–Giemsa, 500? magnification). (b) Prussian blue stain confirms the presence of iron and helps demonstrate the amount of hemosiderin that can be present in liver samples. Hemosiderin likely accumulated secondary to inflammation. Inset image is from the control slide; note the blue-staining iron within this macrophage (Wright–Giemsa, 500? magnification). (Same dog as in Figure 9.28.)
More on the topic Copper:
- Copper
- ELLIPSES
- CHAPTER IX. SIBERIA AND SURROUNDING COUNTRIES.
- References
- Transformation (Specification)
- Impact of Stambheswari on Other Cultures
- Inorganic compounds
- ARCHAEOLOGY AND THE STUDY OF RELIGION: A HISTORICAL OUTLINE
- Mixed inflammation
- PRACTICE EXERCISES