Hyperplasia of the pancreas
Description
Nodular hyperplasia of the exocrine parenchyma is a common incidental finding in old dogs and cats; its presence and severity are correlated with increasing age (Table 8.1) (Meuten, 2002; Newman et al., 2005; Charles, 2007; Zachary & McGavin, 2013).
Hyperplastic nodules should neither be considered as preneoplastic, nor reflect a response to previous pancreatic injury (Meuten, 2002; Newman et al., 2005; Charles, 2007).Pancreatic hyperplastic nodules are typically multiple, raised, smooth, firm, gray or white on cut surface, and of variable size, sometimes larger than normal lobules (Figure 8.9) (Meuten, 2002; Head, 2003; Newman et al., 2005; Charles, 2007). Solitary nodular lesions are unusual and must be differentiated from pancreatic exocrine adenomas, even if the distinction between pancreatic exocrine hyperplasia and adenoma is poorly defined in domestic animals (Meuten, 2002; Newman et al., 2005; Charles, 2007).

Figure 8.9 Pancreatic exocrine nodular hyperplasia from a dog. Hyperplastic nodules are multiple, smooth, well-circumscribed, pale, and raised on the pancreatic surface.
Histopathology
Due to their multiplicity, hyperplastic nodules alternate with normal lobules creating a mosaic of normal and affected lobules (Figure 8.10) (Meuten, 2002; Newman et al., 2005; Charles, 2007).
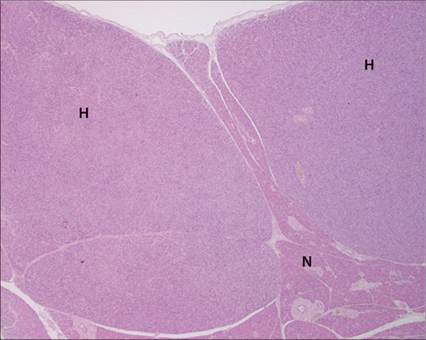
Figure 8.10 Pancreatic exocrine nodular hyperplasia from a cat. Hyperplastic lobules (H) are multiple and larger than adjacent unaffected lobules (N), creating a mosaic. They are slightly compressive and unencapsulated, only delineated by the delicate collagenous septa. Hematoxylin and eosin (?40).
Hyperplastic nodules consist of unencapsulated and minimally or non-compressive small clusters, sheets, or acini of recognizable exocrine pancreatic epithelial cells, with cytoplasmic zymogen granules, and nuclei maintained in a basal location (Figure 8.11) (Head, 2003; Newman et al., 2005; Charles, 2007; Zachary & McGavin, 2013). Affected lobules may be composed of cells larger than normal pancreatic acinar cells, with an abundant brightly acidophilic cytoplasm, rich in zymogen granules, or smaller than normal cells, with a high nuclear-cytoplasmic ratio forming low cuboidal acini and a reduced cytoplasmic content of zymogen granules (Figure 8.12). The cytoplasm may be vacuolated. Mitoses are very rare (Newman et al., 2005; Charles, 2007; Zachary & McGavin, 2013).
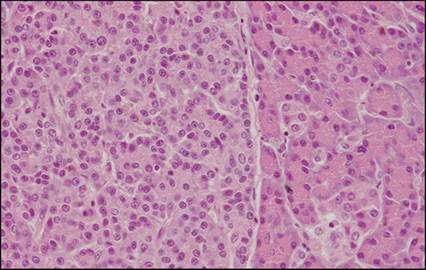
Figure 8.11 Pancreatic exocrine nodular hyperplasia from a cat. In the left part of the micrograph, the hyperplastic nodule is characterized by tightly packed aggregates of recognizable exocrine pancreatic epithelial cells, organized in acini without an obvious lumen: it closely resembles normal counterparts (right of the picture) except for cytoplasmic staining and cell size. Cells are pale, cuboid to pyramidal, with nuclei maintained in a basal location. Hematoxylin and eosin (?400).
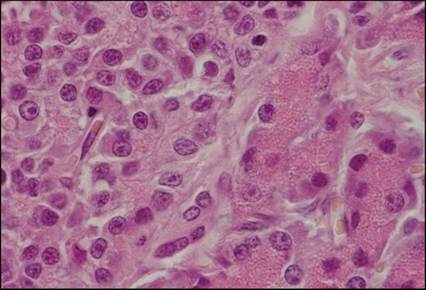
Figure 8.12 Pancreatic exocrine nodular hyperplasia from a cat. At higher magnification, epithelial cells of hyperplastic nodules (left of the picture) are smaller and paler than normal acinar cells (right of the picture), with a higher nuclear to cytoplasmic ratio. The cellular content of zymogen granules is reduced compared to those of adjacent normal exocrine parenchyma. Nuclear alterations are minimal. Hematoxylin and eosin (?1,000).
Ultrasound
Well-defined hypoechoic nodules of various sizes are described in the case of pancreatic nodular hyperplasia (Hecht & Henry, 2007).
Their sonographic appearance can be related to pancreatic endocrine neoplasia (insulinoma), pseudocysts (Penninck et al., 2013), and true cysts, even if the latter are expected to produce posterior enhancement due to their fluid content.Cytology
Cytology of nodular hyperplasia is similar to cytology of adenoma and well-differentiated carcinoma and should always be considered with the ultrasonographic findings and the observation of multiple lesions even if an overlap with neoplastic lesion could exist. FNA are highly cellular (Figure 8.13) and characterized by numerous cohesive cells organized in papillary to acinar structures. Cells appear similar to normal pancreatic epithelial cells with some hyperplastic characteristics such as bigger cells, less granular and more basophilic cytoplasm, higher N:C ratio, bigger and more prominent nucleoli, some anisokaryosis and anisocytosis, and more noticeable binucleations (Figure 8.14) (Bjorneby & Kari, 2002; Andreasen et al., 2010; Borjesson, 2014).
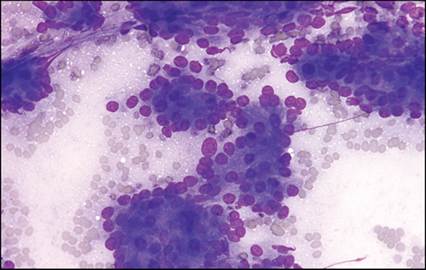
Figure 8.13 Aspirate of a nodular hyperplasia from a cat. Bloody and granular basophilic background associated with numerous cohesive cells organized in acinar and papillary structures. May–Grünwald–Giemsa (?400).
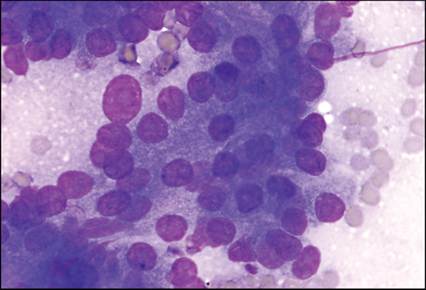
Figure 8.14 Aspirate of a nodular hyperplasia from a cat. Bloody and granular basophilic background associated with acinar cells. The medium- to large-sized cells with a medium to high nuclear to cytoplasmic ratio have a cuboidal to pyramidal outline with indistinct cell borders. Their nuclei are eccentric, round with granular and clumped chromatin and a large prominent nucleolus. Their cytoplasm is basophilic and heterogeneous and characterized by a mild eosinophilic granularity. Anisokaryosis is secondary to an isolated large naked nucleus among a homogeneously sized nucleus population. May–Grünwald–Giemsa (?1,000).
More on the topic Hyperplasia of the pancreas:
- Hantavirus Infection
- Index
- 13 Endocrine Disorders of Pregnancy
- BEHAVIORAL, PHYSIOLOGIC, AND ANATOMIC FEATURES
- BACTERIAL INFECTIONS
- 39 Evaluation of Amenorrhea