Nerves
Two types of nerves should be considered in relation to the middle ear: (1) nerves in transit in close association with the middle ear but destined for a distant location and (2) nerves that play a role in normal function of the middle ear.
All are susceptible to injury by disease of or trauma to the middle ear.Those nerves that are in transit in relation to the middle ear are as follows:
• The sympathetic postganglionic nerves to the eye and orbit from nerve cell bodies located in the cranial cervical ganglion
• The facial nerve and a branch from it (chorda tympani)
• A branch of the glossopharyngeal nerve.
The sympathetic postganglionic nerve fibers are collectively called internal carotid nerves (see Figure 1-11), and they travel as a perivascular nerve plexus along with the internal carotid artery in the petrooccipital canal, which is separated from the middle ear cavity by a thin bony plate in the dog. Chronic infections in the middle ear cavity can erode the bone separating the carotid nerves from the middle ear cavity.
In the cat, the postganglionic sympathetic nerves run through the middle ear cavity submucosally below the septum of the tympanic bulla over the cochlear promontory. Damage to these nerves results in Horner’s syndrome, consisting of miosis (constriction of the pupil) and enophthalmos (recession of the eyeball), which contributes to prolapse of the third eyelid. Ptosis (drooping of the upper eyelid) may also be present.
The facial nerve travels through the bony facial canal (Figure 1-13). As mentioned before, the facial canal is incomplete, exposing this nerve to the middle ear cavity. This can contribute to the involvement of the facial nerve in chronic middle ear infections. Early symptoms of facial nerve involvement may include blepharospasm. Other symptoms, such as drooping of the ear, paralysis of buccal muscles, and spasms of the platysma behind the ear on the affected side, may also be exhibited, depending on the degree of facial nerve involvement.
The chorda tympani, a branch of the facial nerve, runs through the middle ear cavity.
It courses medial to the base of the malleus in the dorsal compartment of the middle ear (see Figures 1-10 and 1-13). The chorda tympani carries preganglionic parasympathetic nerves that synapse in the mandibular and sublingual ganglia to innervate the mandibular and sublingual salivary glands, respectively. This nerve also carries gustatory fibers from fungiform papillae in the rostral two thirds of the tongue. Because taste buds require neurotropic influences to remain functional, damage to the chorda tympani may result in atrophy of fungiform papillae on the affected side.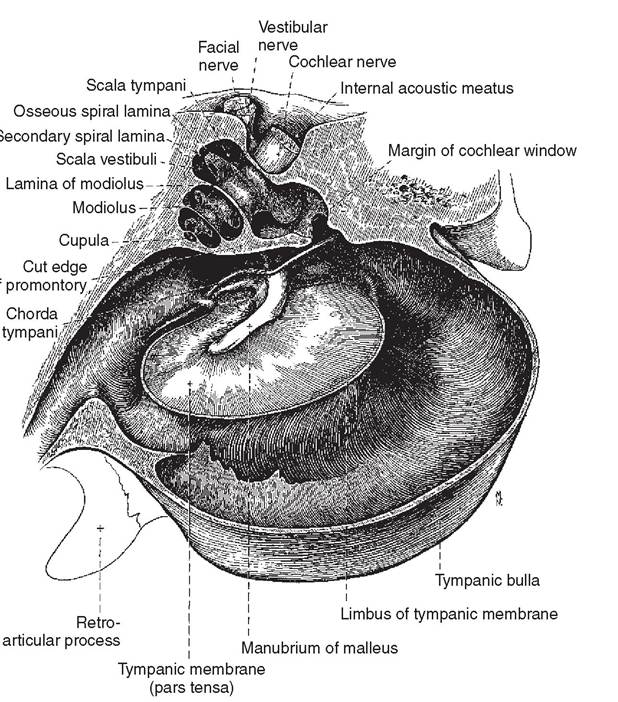
Figure 1-13
Sculpted medial view of the right middle ear and cochlea. (From Evans HE, ed: Miller’s Anatomy of the dog, ed 3, Philadelphia, 1993, WB Saunders.)
The tympanic nerve of the glossopharyngeal nerve supplies the mucous membrane lining of the tympanic bulla. The tympanic nerve gives off the tympanic plexus, which innervates the middle ear cavity (see Figure 1-11).
These nerves may be involved in sensing pressure changes across the tympanic membrane. They may also carry pain sensations from the middle ear cavity. The tympanic nerve itself runs through the middle ear cavity submucosally as the minor petrosal nerve, which mainly carries preganglionic parasympathetic nerve fibers to the otic ganglion. Postganglionic nerve fibers from the otic ganglion innervate the parotid and zygomatic salivary glands. Injury to the tympanic nerve may thus lead to partial loss of salivation on the affected side. The tensor tympani from the mandibular nerve of the trigeminal innervates the tensor tympani muscle. Stapedial nerves from the facial nerve provide motor innervation to the stapedius muscle. The tensor tympani and stapedial nerves are clinically not important.
More on the topic Nerves:
- The normative neurophysiologic data relating to the maturation of peripheral nerves and muscle in children have been greatly expanded in the recent past (1-10).
- The term congenital myopathy is used to describe a group of heterogenous disorders usually presenting with infantile hypotonia due to genetic defects, causing primary myopathies with the absence of any structural abnormality of the central nervous system or peripheral nerves.
- P Keerthi Kundana, Mona Gajre, Alpana Kondekar, Mukesh AgrawalNeurological disorders account for ~15-20% of hospitalizations, which may be divided into three major categories: (a) central nervous system disorders, involving brain and spinal cord, (b) neuromuscular disorders involving peripheral nerves and muscles, and rare disorders of autonomic nervous system.
- Volume Conduction
- Advancements in Upper-Extremity Prosthetics
- Head and Nerve Problems
- Special Considerations for Nerve Conduction Studies
- Nerve Conduction Studies
- Degenerative Changes in the Nervous System
- Cerebellum and Hindbrain
- NEUROMUSCULAR DISORDERS