Vertical Ear Canal
The skin of the vertical canal is approximately 1 mm thick and contains a well- developed dermis and subcutaneous layer. Numerous long, coarse hairs are present along the vertical canal.
Surrounding the hair follicles are numerous sebaceous and ceruminous glands (modified apocrine glands). No eccrine sweat glands are located in the external ear canal. Hairs are most numerous toward the opening of the ear canal; they decrease along the ear canal toward the eardrum. Conversely, the ceruminous glands increase in density in the vertical canal distally.The external acoustic meatus and the skin on the pinna contain numerous adnexal structures and have a significant subcutaneous layer, which can respond to disease. Frequently, the stenotic portion of the ear is limited only to the external

Figure 7-3
Hyperplastic epithelium on the concave pinna closes off the opening to the vertical ear canal.
acoustic meatus (Figure 7-3). In that situation, the otoscope tip may be passed through the stenosis, revealing a normal vertical canal beyond it.
The ear canal of the Shar-Pei has an abundant mucinous dermis under the epithelial layer that increases the thickness and folding of the dermal-epidermal layer. Owing to the anatomically normal thick lining, the lumen diameter in this breed is decreased. The Shar-Pei’s ear canal is thus predisposed to higher humidity and greater glandular secretions, promoting bacterial and yeast colonization.
Anatomically, the vertical canal is more prone to becoming stenotic because of the vascularity and glandular structures found there. The inflammation and edema lead to narrowing of the ear canal. The stenosis prevents drainage of exudates out of the ear canal and complicates therapy by preventing topical medications from achieving therapeutic levels beyond the stenotic portion.
Increases in fluid and air pressure beyond the stenosis can cause excessive pressure on the eardrum, predisposing it to rupture.Inflammation and edema increase the thickness of the subcutaneous layer of the ear canal, leading to stenosis. Chronic otitis externa leads to progressive pathologic changes of the lining epithelium such as hyperkeratosis and hyperplasia (Figure 7-4). The marked thickening of the epithelial layer may significantly reduce ear canal diameter. Increases in the number and size of sebaceous glands (Figure 7-5) and dilated apocrine glands also reduce lumen diameter (Figure 7-6). In addition, pathologic changes that lead to calcification (Figure 7-7) and thickening of the auricular cartilage (especially in American Cocker Spaniels) or to fibrosis and formation of excessive granulation tissue resulting from chronic infection also lead to narrowing of the ear canal lumen (Figure 7-8). Tumors such as ceruminous adenocarcinoma may also occlude the ear canal lumen (Figure 7-9).
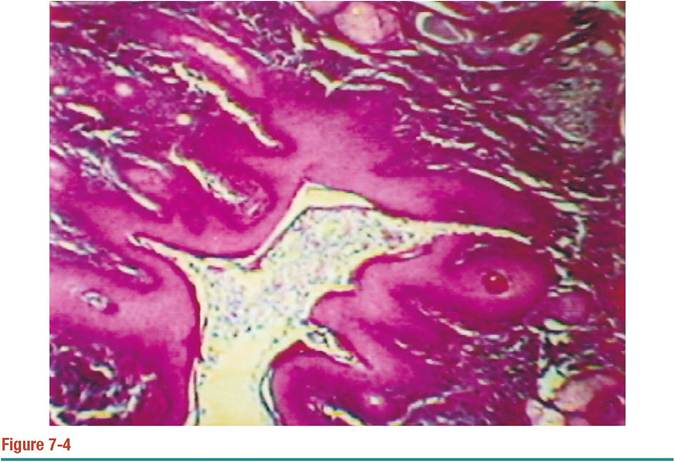
Histopathologic section of an ear canal with extensive fibrosis below a hyperplastic epithelium. Numerous epithelial folds are present and there is an exudate in the stenotic ear canal.

Figure 7-5
Sebaceous hyperplasia usually results in a smooth, stenotic canal. In this Shetland Sheepdog’s ear, the epithelium is also hyperplastic.

Figure 7-6
Ceruminous gland hyperplasia causes a stenosis in the vertical ear canal of this Cocker Spaniel.

Figure 7-7
Radiograph of a stenotic, calcified ear canal in an American Cocker Spaniel. This radiographic sign of pathology indicates a nonreversible, end-stage ear that will require surgical removal.

Figure 7-8
Fibrosis and granulation tissue can result from chronic otitis externa.

Figure 7-9
Cerumen gland adenocarcinomas in an American Cocker Spaniel. This ear was also secondarily infected with Staphylococcus intermedius, which remained until surgery was performed. Laser ablation of these tumors opened up the ear canal.
More on the topic Vertical Ear Canal:
- Organs of Special Sense
- Introduction
- Pinna, or Auricle
- Cases
- The external ear
- Stenosis
- Imaging of the Tympanic Bulla
- Sampling