Diabetes Mellitus
GENERAL PRINCIPLES
• Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. In 2018, diabetes was present in 13.0% of persons age #8805;18 years in the United States and 26.8% of those age 65 and older.
A substantial percentage of affected persons are not diagnosed. Type 2 diabetes mellitus (T2DM) represents 90%-95% of all cases of diabetes, with type 1 diabetes mellitus (TlDM) and other causes representing the remaining 5%-10%.1,2• Patients with diabetes are at risk for microvascular complications, including retinopathy, nephropathy, and neuropathy, and are at increased risk for macrovascular disease.
• T2DM is accompanied by hypertension (approximately 75%) and hyperlipidemia (gt;50%) in adult patients and is considered a “cardiac risk equivalent” because of the excess risk for macrovascular disease, cardiovascular disease (CVD) events, and mortality.3
Classification
Diabetes mellitus is classified into four clinical classes
• T1DM accounts for lt;10% of all cases of diabetes and results from a cellular-mediated autoimmune destruction of the beta (#946;) cells of the pancreas.
• T2DM accounts for gt;90% of all cases of diabetes. T2DM is characterized by insulin resistance followed by reduced insulin secretion from #946; cells that are unable to compensate for the increased insulin requirements.
• Other specific types of diabetes include those that result from genetic defects in insulin secretion or action (known as monogenic diabetes), pancreatic surgery or disease of the exocrine pancreas (cystic fibrosis), endocrinopathies (e.g., Cushing syndrome, acromegaly), or drugs (corticosteroids, antiretroviral, atypical antipsychotics), and diabetes associated with other syndromes. Pancreatic diabetes is now commonly referred to as type 3c diabetes.
• Gestational diabetes (GDM) is glucose intolerance with onset or diagnosis during pregnancy. The prevalence of GDM depends on the criteria used for diagnosis and varies by age and ethnic group (generally from 5% to 6% of pregnancies to 15%-20% of pregnancies). Diagnostic criteria for GDM vary based on practice location with a two-step method (50-g, 1-hour screen followed by 100-g, 3hour oral glucose tolerance test [OGTT]) used in the United States and a one-step method (75-g, 2-hour OGTT) more common internationally.4 About 50% of women with GDM will develop T2DM in the ensuing 5-10 years, and all remain at an increased risk for the development of T2DM later in life.
î All patients with GDM should undergo diagnostic testing 4-12 weeks postpartum with a 2-hour OGTT or fasting plasma glucose and every 1-3 years thereafter with either test or an A1C to determine whether abnormal carbohydrate metabolism has persisted or is recurrent.
î Weight loss, exercise, and breastfeeding are encouraged to decrease the risk of persistent prediabetes or T2DM after delivery.
DIAGNOSIS
• Progression from impaired fasting glucose or impaired glucose tolerance to T2DM occurs at the rate of 2%-22% (average, about 12%) per year depending on the population studied.
• Lifestyle modification, including a balanced hypocaloric diet to achieve 7% weight loss in overweight patients and regular exercise of #8805;150 min/wk, is recommended for persons with prediabetes to prevent progression to T2DM.5
• Metformin may be considered in patients with prior GDM, those with body mass index (BMI) #8805;35, age lt;60 years, or those with progressive hyperglycemia.
• Diagnostic criteria for prediabetes and diabetes are listed in Table 23-1.
TABLE 23-1
DIAGNOSIS OF DIABETES
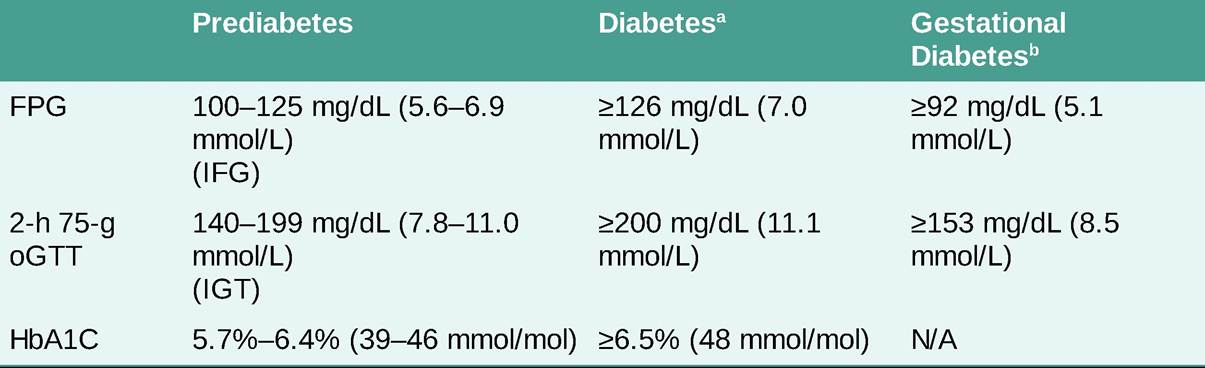
FPG, fasting plasma glucose; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; HbA1C, hemoglobin A1C; oGTT, oral glucose tolerance test.
aRequires two tests to confirm diagnosis unless random glucose #8805;200 mg/dL (11.1 mmol/mol) with polyuria, polydipsia. bThese are IADPSG guidelines used internationally. A single abnormal value is considered diagnostic of gestational diabetes on these guidelines. 1-h post 75-g glucose load #8805;180 mg/dL (10 mmol/L) can be used for diagnosis of GDM on these guidelines as well. In the United States, a two-step method is still most common: nonfasting 1-h post 50-g glucose challenge #8805;140 mg/dL (7.8 mmol/L) (some centers use 130 mg/dL [7.2 mmol/L] or 135 mg/dL [7.5 mmol/L]) necessitates a 3-h 100-g oGTT and Carpenter and Coustan Criteria are used for diagnosis (exceeding 2+ of the following thresholds: fasting #8805;95 mg/dL [5.3 mmol/L], 1-hour #8805;180 mg/dL [10 mmol/L], 2-hour #8805;155 mg/dL [8.6 mmol/L], 3-hour #8805; 140 mg/dL [7.8 mmol/L]).
TREATMENT
• Goals of therapy are alleviation of symptoms, achievement of glycemic control, blood pressure and lipid targets, and prevention of acute and chronic complications of diabetes.
• Glycemic control recommendations are the same for T1DM and T2DM outside of pregnancy: Fasting and preprandial capillary blood glucose (BG) 80-130 mg/dL (4.4-7.2 mmol/L) and postprandial capillary BG lt;180 mg/dL (lt;10 mmol/L). The American Diabetes Association and American Association of Clinical Endocrinologists now recommend a customized A1C goal based upon an individual’s age and comorbidities. Goals for younger individuals without comorbidities can be lt;6.5% (48 mmol/mol) while individuals who are over 65 and have cardiovascular comorbidities or with limited life expectancy may reasonably aim for A1C lt; 8% (64 mmol/mol).6,7 A1C lt;6.5%-7% (lt;48-53 mmol/mol) has been associated with the lowest risk for microvascular complications in patients with T1DM and T2DM.8,9 However, the customized goals recognize that it is also important to avoid frequent hypoglycemia.
• To minimize the risk of fetal macrosomia and neonatal hypoglycemia, glycemic goals in pregnancy are fasting BG 70-95 mg/dL (3.9-5.3 mmol/L), 1 hour postprandial #8804; 140 mg/dL (7.8 mmol/L), 2-hour postprandial #8804;120 mg/dL (6.7 mmol/L).
• Consensus on continuous glucose monitoring goals for type 1 and 2 diabetes include gt;70% time in range (70-180 mg/dL; 3.9-10.0 mmol/L) with lt;4% below 70 mg/dL (3.9 mmol/L), lt;1% below 54 mg/dL (3.0 mmol/L), lt;25% above 180 mg/dL (10 mmol/L), and lt;5% above 250 mg/dL (13.9 mmol/L). In pregnancy, goal time in range for type 1 diabetes is gt;70% (63-140 mg/dL; 3.5-7.8 mmol/L).10
• Intensive diabetes therapy leading to very tight glycemic control in patients with risk factors for CVD has been associated with increased mortality in two studies,11,12 but not in others.13 Hypoglycemia was implicated as the cause of higher mortality in one of the studies.
• The blood pressure target for patients with diabetes is lt;140/90 mm Hg, but a lower goal of lt;130/80 mm Hg may be considered for younger patients or those at high risk of CVD (ASCVD 10 years risk #8805; 15%). The use of either an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) is recommended as first-line therapy. Thiazide diuretics and calcium channel blockers are reasonable second-line agents. Two agents should be started in individuals with blood pressure #8805; 160/100 or not at goal on one agent.
• High-intensity statin therapy (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) is recommended in patients with diabetes age 40-75 with CVD risk factors. Moderate-intensity statin therapy can be considered in patients age 40-75 with no other CVD risk factors and in patients with age lt;40 or gt;75 with CVD risk factors.
• The low-density lipoprotein (LDL) goal for patients with diabetes and CVD is lt;70 mg/dL (3.9 mmol/L). If that goal is not achieved with statin therapy, the addition of either ezetimibe or a PCSK9 inhibitor is advised.
• Aspirin therapy should be recommended in patients with diabetes and cardiovascular disease. Low doses (75-162 mg) are appropriate. Aspirin may be considered for primary prevention in individuals with diabetes after considering potential benefit and risk of bleeding.
Clopidogrel (75 mg/d) may be used for secondary prevention in individuals with aspirin allergy.• Individuals with diabetes are at high risk for nonalcoholic fatty liver disease. Weight loss is recommended as first-line therapy for treating this comorbidity (see Chapter 19, Liver Diseases).
• Assessment of glycemic control consists of the following:
î Self-monitoring of blood glucose (SMBG) is recommended for all patients who take insulin and provides useful information for those on noninsulin therapies. Patients using multiple daily injections or insulin pumps should test their blood glucose three or more times daily. Less frequent testing may be appropriate for those on noninsulin therapies. Although most SMBG is done before meals and at bedtime, periodic testing 1-2 hours after eating may be necessary to achieve postprandial glucose targets.
î Continuous glucose monitoring (CGM) has been shown to reduce A1C in adults older than 25 years and reduce hypoglycemia in patients of all ages on intensive insulin therapy. CGM measures interstitial glucose, which provides a close approximation of BG values. Hypoglycemia and hyperglycemia alarms may help patients with widely fluctuating BG levels or hypoglycemia unawareness. Some of the CGM devices are approved for insulin dosing and may supplant the need for SMBG.14
o A1C provides an integrated measure of BG values over the preceding 2-3 months. A1C should be obtained every 3 months in patients not at goal, when either diabetes therapy or clinical condition changes, or twice yearly in well-controlled patients. A1C should confirm results of SMBG or CGM, and discordant values should be investigated. An A1C level that is higher than expected should be evaluated by a diabetes educator to ensure meter accuracy, appropriate technique, and frequency of testing. When the A1C is lower than expected, blood loss, transfusion, hemolysis, and hemoglobin variants should be considered. The correlation between A1C and mean plasma glucose is sufficiently strong that laboratory reports may include both the A1C result and the estimated average glucose.
î Ketones can be detected in a fingerstick blood sample by measuring #946;-hydroxybutyrate with a handheld meter. Urine ketones can be qualitatively identified, using Ketostix or Acetest tablets. Patients with T1DM should test for ketones during febrile illness, for persistent elevation of glucose (gt;300 mg/dL [16.7 mmol/L]), or if signs of impending diabetic ketoacidosis (e.g., nausea, vomiting, abdominal pain) develop.
MANAGEMENT
Comprehensive diabetes management includes coordinated diet, exercise, and medication plans. Patient education in medical nutrition therapy, exercise, SMBG, medication use, and insulin dosing and administration is integral to the successful management of diabetes.
Medical Nutrition Therapy
• Medical nutrition therapy includes dietary recommendations for a healthy, balanced diet to achieve adequate nutrition and maintain an ideal body weight.15
• Caloric restriction is recommended for overweight individuals, with individualized targets that may be as low as 1000-1500 kcal/d for women and 1200-1800 kcal/d for men depending on activity level and starting body weight, and goal weight loss of at least 5%.
• No ideal distribution of calories from fat, protein, and carbohydrate has been defined. Multiple eating patterns such as Mediterranean, plant-based, DASH diet, or low-carbohydrate diet may be used to meet dietary goals for individuals with diabetes.
• A focus on avoiding sugar-sweetened beverages and optimizing nonstarchy vegetable and whole grain intake is appropriate.
• “Carbohydrate counting” is a useful skill for patients on intensified insulin therapy who adjust insulin doses based on the carbohydrate content of meals and snacks.
Exercise
Exercise improves insulin sensitivity, reduces fasting and postprandial BG levels, and offers numerous metabolic, CV, and psychological benefits in patients with diabetes.
• In general, 150 min/wk of moderate to vigorous aerobic activity is recommended as part of a healthy lifestyle and has been shown to assist with the prevention and management of T2DM in adults. Resistance exercise 2-3 times/wk is also important.
• Patients may need individualized guidance regarding exercise, and they are more likely to exercise when counseled by their physician to do so.
• Prolonged sitting over 30 minutes at a time should be avoided.
More on the topic Diabetes Mellitus:
- Type 2 Diabetes
- 4 Preconception Counseling and Prenatal Care
- DIABETES INSIPIDUS
- Endocrine pancreas
- Intraocular structures
- Macrovascular Complications of Diabetes Mellitus
- Adrenal gland neoplasia
- Focal Segmental Glomerulosclerosis
- Pancreatic tumors
- Endocrine pancreas