Ovulation and ovarian function
Control of the hypothalamic-pituitary axis
The hypothalamus is part of the diencephalon. It is separated from the thalamus by the hypothalamic sulcus. Its external boundaries are rostrally the optic chiasm, laterally the optic tract, and posteriorly the mammillary bodies.
Its rostral boundary is a line through the optic chiasm, lamina terminalis, and anterior commissure and the caudal boundary extends from the posterior commissure to the caudal limit of the mammillary body. Dorsolaterally, the hypothalamus extends to the medial edge of the internal capsule (Figure 1.1) (2). The hypothalamus is associated with visceral, endocrine, autonomic, affective, and emotional behaviour.
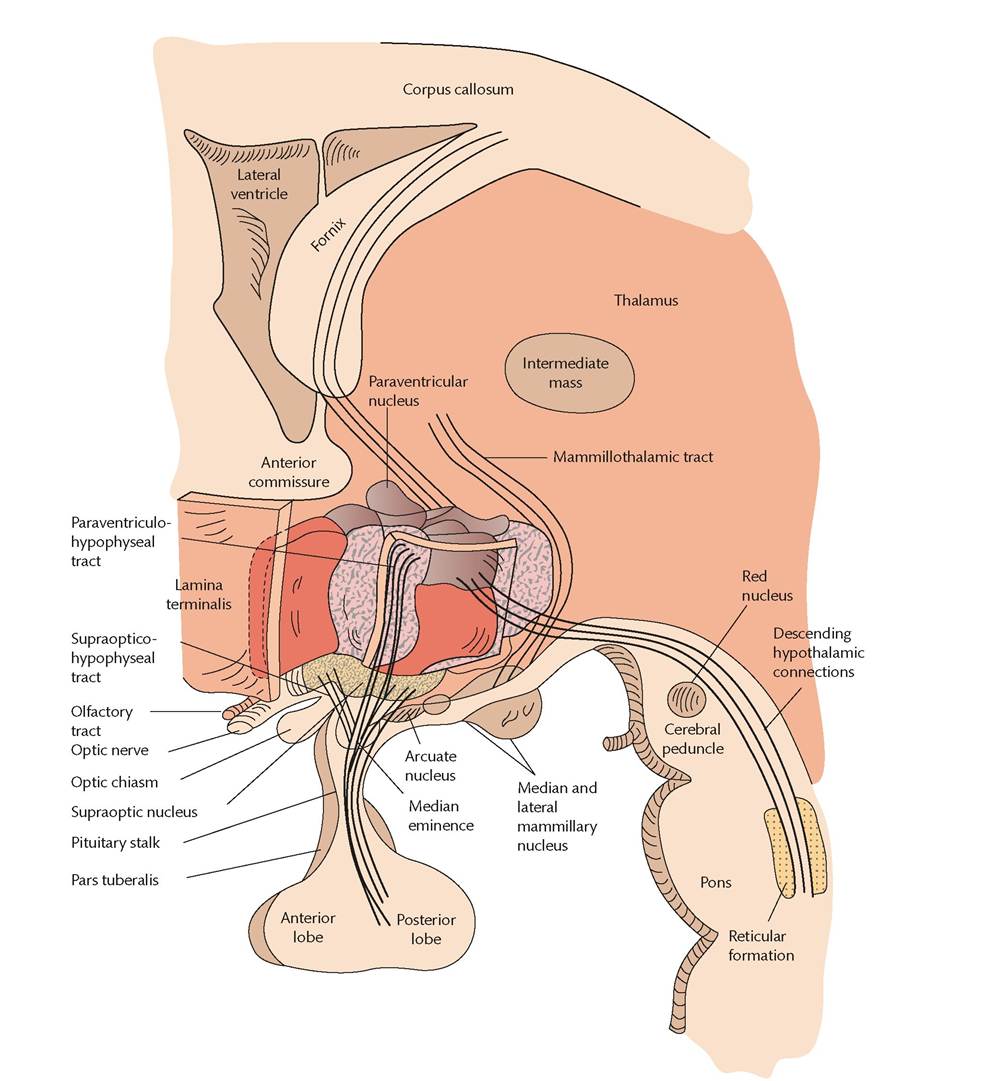
Figure 1.1 The hypothalamic nuclei and hypothalamic-hypophyseal tracts in relation to the thalamus, ventricular system, and brainstem.
Reproduced from Ignacio Bernabeu, Monica Marazuela, and Felipe F. Casanueva, General concepts of hypothalamus-pituitary anatomy, in: Oxford Textbook of Endocrinology and Diabetes 2e (eds: John Wass et al.), Oxford University Press, 2011, with permission from Oxford University Press.
The anterior pituitary is connected to the hypothalamus through a portal system. Hormones synthesized in the hypothalamus are transported to the nerve terminals on the hypophyseal portal capillaries. Hormones released into the hypophyseal portal system are transported to the anterior lobe of the pituitary. The posterior lobe of the pituitary consists of nerve terminals which lie in the supraoptic and paraventricular nuclei of the hypothalamus. Oxytocin and vasopressin are synthesized by the posterior pituitary.
Actions of pituitary and ovarian hormones
Gonadotropin-Teleasinghormone (GnRH) is synthesized in the preoptic area of the hypothalamus and is transported via portal vessels to the anterior pituitary where it stimulates the gonadotrophs to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
These glycoproteins share a common alpha-subunit and a specific betasubunit. They control the steroid synthesis of the testes and ovaries.Oestrogen and progesterone are the major hormones secreted by the ovarian follicles and the corpus luteum (Figure 1.2).
Ovulation
A rise in FSH secretion stimulates the growth and differentiation of preantral and antral follicles, which in turn stimulates oestrogen secretion with a peak approximately 1 day before ovulation. Then, the mid-cycle surge occurs (3) and is associated with a change from negative feedback control of LH secretion by ovarian hormones to
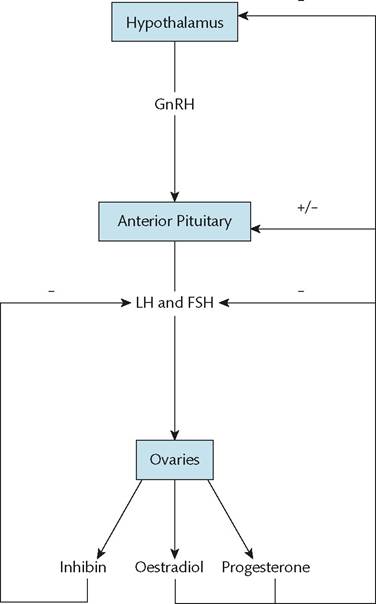
Figure 1.2 Hypothalamic-pituitary-ovarian axis.
Reproduced from S. Arulkumaran, Menstrual disorders, in: Training in Obstetrics and Gynaecology (eds. Ippokratis Sarris, Susan Bewley and Sangeeta Agnihotri), Oxford University Press, 2009, with permission from Oxford University Press.
a positive feedback, resulting in a tenfold rise in serum LH and a smaller increase in FSH concentrations. The LH surge leads to substantial changes in the ovary. The oocyte in the dominant follicle completes its first meiotic division. The oocyte is subsequently released from the follicle at the surface of the ovary (4).
Before the release of the oocyte, the surrounding granulosa cells luteinize and produce progesterone. As a result, LH pulses become less frequent by the end of the surge (Figure 1.3).
The increasing serum progesterone concentrations have an effect on the endometrium, leading to cessation of mitoses and ‘organization’ of the glands.
Endometrial cycle
The average duration of the adult menstrual cycle is 28-35 days. The first day of menses represents the first day of the cycle. The cycle is then divided into two phases: follicular and luteal. The follicular
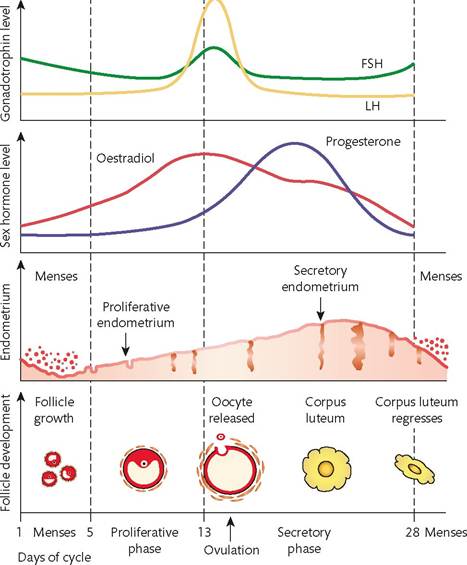
Figure 1.3 The hormonal and endometrial axis of the human menstrual cycle.
After menstruation, rising levels of oestrogen exert a negative feedback, reducing follicle-stimulating hormone (FSH) release. Towards mid cycle, still higher levels of oestrogen then exert a positive feedback, causing a sudden peak release of luteinizing hormone (LH), which induces ovulation. An increased level in FSH also occurs. The endometrium during this phase has a thin surface epithelium and the glands are straight, short, and narrow (proliferative/follicular). In the luteal phase, LH levels maintain the corpus luteum, the source of progesterone. The endometrial glands become more tortuous during this phase (secretory/luteal) with secretion in the lumen and increasing fluid separating the stromal cells. If an embryo fails to implant, the corpus luteum deteriorates after about 7 days, with a resulting fall in progesterone and oestrogen concentrations.Reproduced from S. Arulkumaran, Menstrual disorders, in: Training in Obstetrics and Gynaecology (eds. Ippokratis Sarris, Susan Bewley and Sangeeta Agnihotri), Oxford University Press, 2009, with permission from Oxford University Press. phase begins with the onset of menses and ends on the day before the LH surge. The luteal phase begins on the day of the LH surge and ends at the onset of the next menses. The follicular phase lasts approximately 14-21 days and the luteal phase 14 days. Changes in the intermenstrual interval are primarily due to changes in the follicular phase. The luteal phase remains relatively stable. There is significantly more cycle variability during the first years after menarche and the 10 years before menopause. Menstrual cycle length peaks at the age of 25-30 years and then gradually declines. Between the ages of 20 and 40 years, there is relatively little cycle variability. Women in their 40s may have slightly shorter cycles (5).
During the menstrual cycle, endometrial changes include a proliferative phase and a secretory phase. The proliferative phase is characterized by an increased rate of mitotic division of endometrial glandular cells under the influence of oestradiol, leading to proliferation.
The secretory phase is characterized by secretory activity following further proliferation under the influence of oestradiol and progesterone.Luteinization of corpus luteum occurs 14 days after ovulation in the absence of conception. A rise in FSH is induced by the loss of negative feedback from oestradiol and progesterone, resulting in the start of another cycle. If, however, conception occurs, luteinization does not occur and the corpus luteum is maintained by human chorionic gonadotropin.
Puberty and menopause
Puberty is a process of physical and hormonal changes resulting in sexual maturity and capability of sexual reproduction. The two main Thelarche is the appearance of breast tissue. Menarche is the onset of menstrual cycles. This is caused by the action of oestradiol on the endometrium and usually is not associated with ovulation. Spermarche is the onset of sperm production. Pubarche is the appearance of pubic hair, primarily due to the effects of androgens from the adrenal gland. The term also refers to the appearance of axillary hair (Figure 1.4).
In puberty, the increased frequency and amplitude of GnRH pulses stimulates secretion of FSH and LH and activates gonadal steroidogenesis.
Leptin is secreted by adipose tissues and along with kisspeptin plays a role in the onset of puberty. Menopause is defined as the permanent cessation of menstruation. It is an oestrogen- and progesterone-deficient state with an increase in the secretion of FSH and LH. The cessation of menstrual periods occurs as the ovary no longer contains follicles which are responsive to FSH. It is diagnosed retrospectively after 12 months of amenorrhea without any other cause (Figure 1.5).
Lack of oestrogen causes vasomotor symptoms including hot flushes and night sweats as well as mood swings and depression. Long-term effects include lower genital tract atrophy, osteoporosis, changes in lipid metabolism, and an increased risk of cardiovascular disease (6). Menopause usually occurs between 45 and 55 years of
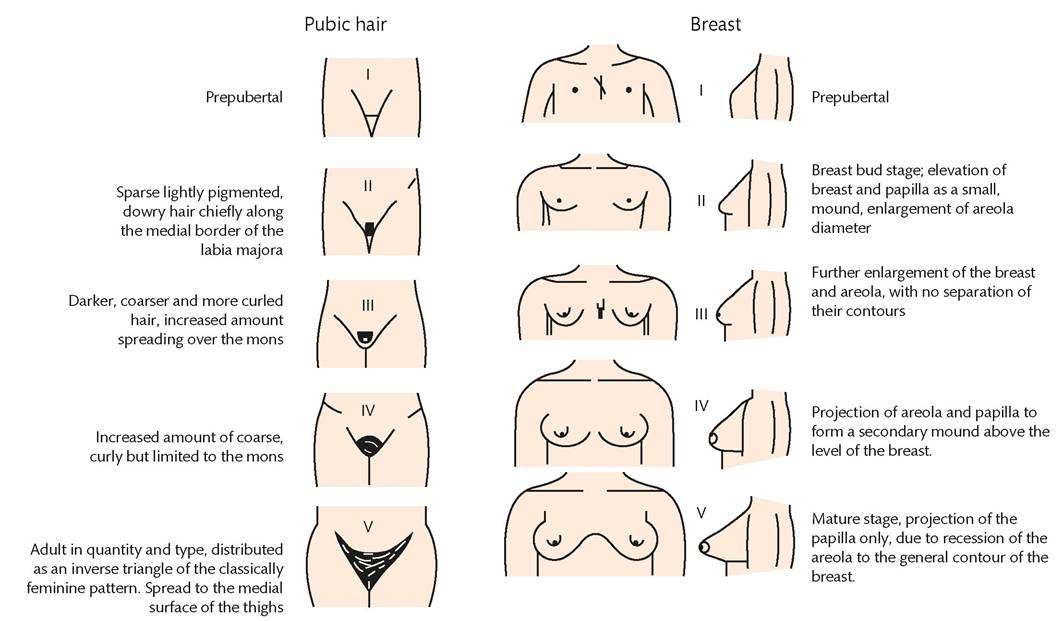
Figure 1.4 Marshall and Tanner stages of breast and pubic hair development.
Reproduced from McVeigh E, Homburg R, and Guillebaud J. Oxford Handbook of Reproductjve Medicine and Family Planning, Oxford University Press, 2008, with permission from Oxford University Press.
Age (years)
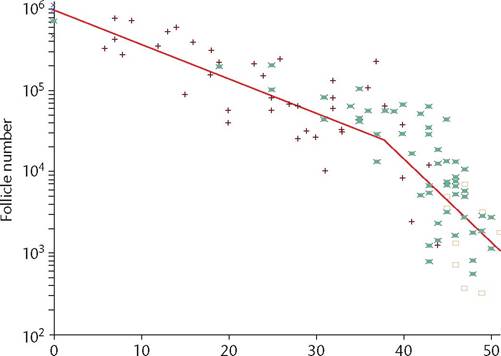
Figure 1.5 Decline in primordial follicle number with age.
Reproduced from Faddy MJ, Gosden RG. A mathematical model of follicle dynamics in the human ovary. Hum Reprod. 1995; 10: 770-5 with permission from Oxford University Press.
age. In the United Kingdom, the average age of menopause is 51. Menopause before the age of 40 years is considered abnormal and is referred to as primary ovarian insufficiency (premature ovarian failure).
The transition to menopause, or perimenopause, is characterized by irregular menstrual cycles (7) and hormonal fluctuations, and a variable frequency and severity of symptoms such as hot flashes, sleep disturbances (8), mood changes, and vaginal dryness. It begins on average 4 years before the final menstrual period (9).
More on the topic Ovulation and ovarian function:
- Menstrual physiology
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- Diagnostic categories in infertility
- Chapter 37 Reproductive Cycles
- Obesity and preconceptional counselling
- Treatment of endometriosis-associated infertility
- 43 Menopause
- Chapter 50 Ovarian and Adnexal Disease
- Pathophysiology of polycystic ovary syndrome
- Chapter 41 Menopause