10.33 MALARIA MYCOPLASMA INFECTIONS
Two mycoplasmal infections are of interest in human disease - M. pneumoniae and Genital mycoplasma, i.e. M. hominis and Ureaplasma urealyticum.
M. pneumoniae (Eaton agent), the smallest self-replicating organism, is the commonest cause of community-acquired pneumonia in schoolchildren.
Epidemiology: Infection is acquired via droplets from infected host, though development of clinical disease depends on age and immune status. Overt illness is unusual before 3-4 years of age, while children with immunocompromised illness or sickle cell disease are at risk for serious disease.
Clinical spectrum: Primary atypical pneumonia is the commonest mycoplasmal illness, responsible for gt;1/3rd cases of community-acquired pneumonia in school children. Other rare manifestation include: (a) upper respiratory illnesses, e.g. pharyngitis, otitis or sinusitis,
(b) airway illnesses, e.g. croup, bronchiolitis, and
(c) exacerbation of asthma. Mycoplasma infections may also lead to extra-respiratory complications after 2-3 weeks of respiratory illness, due to autoimmune mechanisms, e.g. (a) Steven-Johnson syndrome, (b) neurological disease, e.g. aseptic meningitis, transverse myelitis, Guillain-Barre syndrome, cerebellar ataxia, and (c) autoimmune hemolytic anemia.
Diagnosis usually rests on serology, i.e. elevated cold agglutinin titers (gt;1:64) or positive IgM-ELISA test. Cultures take gt;1 week for results and molecular diagnostic tests, e.g. PCR are not commercially available. Treatment of choice is Macrolides, e.g. Clarithromycin (PO 15 mg/kg/day q12hr for 10 days) or Azithromycin (PO 10 mg/kg/day q24hr for 5 days), with nearly 100% success rate. In rare resistant case, tetracyclines or fluoroquinolones may be used.
Genital mycoplasma (M. hominis and U. urealyticum) are common colonizers of genitourinary tract in post-pubertal adults, rarely transmitted to newborns or children via sexual abuse, genital-hand-genital contact, during vaginal delivery or in presence of chorioamnionitis.
Neonatal infection with genital mycoplasma has been attributed to abortions, stillbirths, prematurity and rarely, neonatal respiratory disease.
Adolescent infection may be asymptomatic or presents with non-gonococcal urethritis in males and vaginitis, cervicitis and pelvic inflammatory disease in females.
Diagnosis of pathogenic infection is difficult due to high colonization rate in normal population.
Treatment of choice is single dose Azithromycin, indicated only in symptomatic cases with pure mycoplasma culture.
Malaria continues to be a major public health problem in India and has acquired new dimensions due to (a) resurgence in previous low-endemic areas, (b) increasing proportion of severe P. falciparum cases, and (c) emergence of drug-resistance.
India aims to eliminate malaria with 2030, with zero indigenous cases in the entire country, maintain malaria-free status in areas where transmission has been interrupted, and prevent re-introduction of malaria, as also recommended by WHO Global Technical Strategy for Malaria 2016-2030.
Magnitude of malaria in a community is usually measured as annual parasite incidence (API), i.e. number of smear-positive cases per year per 1000 population. Recent years have witnessed major changes in malarial epidemiology in India, as follows:
• Significant decline in the incidence of disease with API of 0.12 in 2021 (vs 2.12 in 2001).
• Predominance of falciparum (Pf) infection, accounting for ~57% of all malaria cases (2022).
• Wide regional differences, with maximum cases in Chhattisgarh, Odisha, Jharkhand and North-eastern states (2022).
• Alarming rise in drug-resistance Pf cases, specially to Chloroquine (~40%) or Pyrimethamine (~10-20%). Partial chloroquine resistance in vivax (Pv) malaria is also emerging.
Epidemiology: Human malaria is caused by four species of Plasmodium-an obligate intracellular protozoon: P. vivax (benign tertian malaria), P. falciparum (malignant tertian malaria), P.
malariae (Quartan malaria) and P. ovale. In India, P. malariae accounts for lt;1% cases in Tumkar and Hassan districts of Karnataka, and P. ovale is extremely rare. Few cases of malaria due to P. Knowlesi have been reported in south-east Asia, but not in India.Reservoir: Infected humans are the only known reservoir of infection, except probably chimpanzees in tropical Africa. Infected person is communicable only if gametocytes are present in peripheral blood, which appear on 4-5th day in Pv and 10-12th day in Pf, after onset of fever.
Transmission: Mosquito as a vector for malaria transmission was first identified in 1897 by Ronal Ross from Hyderabad, India. Malaria is transmitted by the bites of infected female anopheline mosquitoes, except rare cases of congenital malaria (transplacental infection), transfusion malaria (infected blood/products) or needle-infection in drug-users. Six species of female anopheline are known to transmit malaria. In India, maximum transmission occurs by A. stephensi (urban slums) or A. culcifacies (rural areas) and rarely by A. minimus (North-East states). Vector typically breeds on stagnant water, e.g. ponds, cisterns, fountains and overhead tanks.
Host factors: Malaria is common in all age-groups and in males. Since all infected mosquito-bites do not cause clinical disease, host characteristics seem to play important role, as follows:
• Newborns are relatively protected, due to presence of high fetal hemoglobin levels (relatively malaria resistant) and transplacental antibodies.
• Inherent immunity is present in some people, probably due to: (a) genetic immunity, dependent on HLA type, (b) absence of surface receptors for merozoites on RBC membrane, or (c) presence of hemoglobinopathies, e.g. sickle cell disease, etc., which resist parasitic entry, impede in vivo development, or facilitate their removal.
• Acquired resistance due to earlier attacks in endemic population. Most severe malaria occurs in non- immune persons, e.g.
travelers to endemic regions.Environmentalfactors relate to vector population and activity. Malaria is more prevalent in:
• Areas with suitable vector-breeding conditions, e.g. villages and urban slums, heavy rainfall regions, e.g. north-east states, construction sites and man-made breeding sites, e.g. burrow pits, garden pools and irrigation channels (man-made malaria).
• Warm-humid climate from July to November, due to increased vector-activity. Malaria is uncommon in hilly regions due to cold weather, unsuitable for mosquito survival.
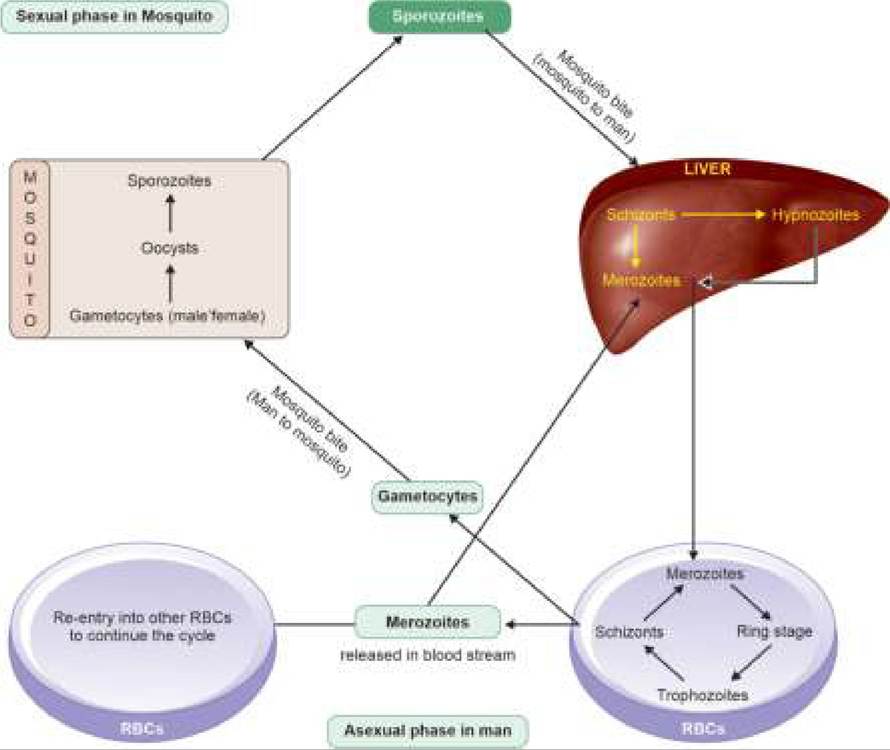
Life-cycle of parasite completes in two hosts—asexual phase in man and sexual phase in mosquito (Fig. 10.17).
Asexual phase (in man) begins with infected mosquito bite and entry of sporozoites in blood. Most of these sporozoites invade hepatocytes for asexual reproduction, though some are destroyed by phagocytosis in immune people. Asexual phase may be divided into:
a. Hepatic (pre-#8725;exo-erythrocytic) phase: During incubation period, sporozoites within liver cells develop into hepatic schizonts, which eventually rupture to release thousands of merozoites (~2000-15,000 in Pv and gt;40,000 in Pf) in blood. In Pv infection, some schizonts remain dormant in the hepatocytes (hypnozoites) to mature and rupture later, leading to late relapses (exo-erythrocytic phase). This phase is absent in Pf infections and congenital/transfusion malaria (no relapse).
b. Erythrocytic phase: Liberated merozoites from liver invade RBCs by attaching themselves on cell-surface receptors and develop intracellularly through many developmental stages, e.g. ring stage gt; trophozoites gt; erythrocytic schizonts and again as merozoites. Infected RBC ruptures to release them in peripheral blood, with reappearance of fever. Subsequent course of merozoites is:
- Re-infection of other RBCs and re-cycling till d ev e l op m en t o f a d e qu at e na tu r al i m m u ni t y. Each erythrocytic cycle takes ~42 hrs (~72 hrs in P. malariae), responsible for typical periodicity of fever, i.e.
tertian malaria (Pv, Pf) or quartan malaria (P. malariae).- Re-entry of some merozoites (except in Pf) into hepatocytes to re-start hepatic/exo-erthrocytic phase, responsible for relapses.
- Development into sexual forms, i.e. micro (male) or macro (female) gametocytes, for infection of other mosquitos.
Sexual phase (in mosquito) involves fusion of male and female gametocytes to form zygote in the stomach of mosquito that develops further as sporozoites and enters into salivary glands, ready to inoculate next human host. Pathogenesis: Clinical differences in the severity of illness in Pv and Pf infection mainly relate to magnitude of parasitemia, i.e. number of RBCs infested. As many as 30-40% of RBCs may be simultaneously infected in severe Pf malaria, as compared to lt;5% parasitization in Pv infections. Further, Pv invades only the younger RBCs, while Pf also infects senescent erythrocytes.
Important factors in pathogenesis of malaria are:
• Hemolysis of parasitized RBCs, leading to febrile episodes and anemia;
• Increased cytoadherence of parasitized RBCs, leading to intravascular clogging and hypoxic-ischemic tissue injury. Falciparum infested erythrocytes tends to adhere to uninfected RBCs (rosetting) to promote cytoadherence, specially in severe cerebral malaria.
• Immunological injury with hypergammaglobulinemia, immune-complex formation and release of pro- inflammatory cytokines, (e.g. interleukins and TNF-#945;), which precipitate or aggravate tissue hypoxia/injury. Immune response to malaria is slow, incomplete and
not life-long, due to antigenic diversity of the parasite. However, repeated exposures tend to reduce the severity of disease due to partial immunity in older population of endemic regions.
Clinical manifestations of malaria begin after an incubation period of ~ 9-14 days in Pf and ~ 12-17 days in Pv infection; and depend on the magnitude of parasitized RBCs as well as immune status of host. In endemic regions, e.g. India, even 20-30% parasitemia may be asymptomatic in older cases due to acquire immunity after repeated exposures.
Some important manifestations of malaria are as follows:Classical malaria, is characterized by typical periodicity of intermittent fever. Each episode evolves through following three stages:
a. Cold stage, i.e. sudden chills and rigors for ~ 10-15 minutes, followed by,
b. Hot stage, i.e. sudden rise of temperature, lasting for 2-3 hours, followed by,
c. Wet stage, i.e. profuse sweating, when fever comes down by lysis.
Fig. 10.17: Life cycle of malaria parasite.
On examination, mild splenomegaly and pallor is common.
Severe malaria is more common in non-immune population, almost always caused by Pf infection and defined as presence of any of the manifestations enumerated in Table 10.53. Cerebral malaria is the commonest and most serious presentation of severe malaria in children (Ch 18.11.4). Severe malaria due to vivax malaria is rare, but has been reported. Diagnostic criteria for severe Pv malaria are similar to those for severe Pf malaria, but with no definite parasite thresholds.
Chronic malaria is a common problem in endemic region due to relapses (in Pv infection) or recurrent infections. Armed with partial immunity, these cases often presents with intermittent bouts of mild febrile episodes but progressive splenomegaly.
Neonatal malaria is uncommon due to high fetal hemoglobin (relatively resistant), and may be (a) Congenital or transplacental, due to maternal infection in last week of gestation, or (b) Acquired due to mosquito bite in early neonatal period.
TABLE 10.53: WHO criteria for severe falciparum malaria (2023 update)
• Impaired consciousness (Blantyre coma score lt;3)
• Generalized prostration (inability to sit/stand/walk)
• Hypoglycemia (Blood sugar lt; 40 mg/dl)
• Recurrent seizures (#8805;3 in 24 hours)
• Metabolic acidosis (HCO3 lt;15 or lactate gt;5 mmol/L)
• Severe anemia with PC gt;10000#8725;#956;l (Hb #8804;5 or Hct #8804;15)
• Recurrent or prolonged bleeding
• Jaundice with PC gt;100000/pl (bilirubin gt;3 mg/dl)
• Hyperparasitemia (gt;10%)
• Pulmonary edema (On X-ray or SaO2 lt;92%)
• Circulatory shock (SBP lt;70 mm Hg or CRT #8805;3 sec.)
• Renal failure (S. creatinine gt;3 mg/dl)
PC: Parasite count, RD: Respiratory distress, CRT: Capillary refill time, SBP: Systolic blood pressure
These cases presents with septicemia-like manifestations, e.g. poor feeding, sluggish activity, pallor, jaundice, diarrhea/vomiting and hepatosplenomegaly. Antenatal maternal infection is also associated with intrauterine fetal death, premature labor and IUGR. Although d/d with acquired neonatal malaria is difficult, congenital malaria is characterized by: (a) onset within 7 days of life, (b) absence of exo-erythrocytic phase with no relapses and (c) positive maternal/placental blood smear.
Diagnosis of malaria depends on the peripheral smear or a rapid diagnostic test, though collaborative hematological findings may support the diagnosis in a clinically suspected case.
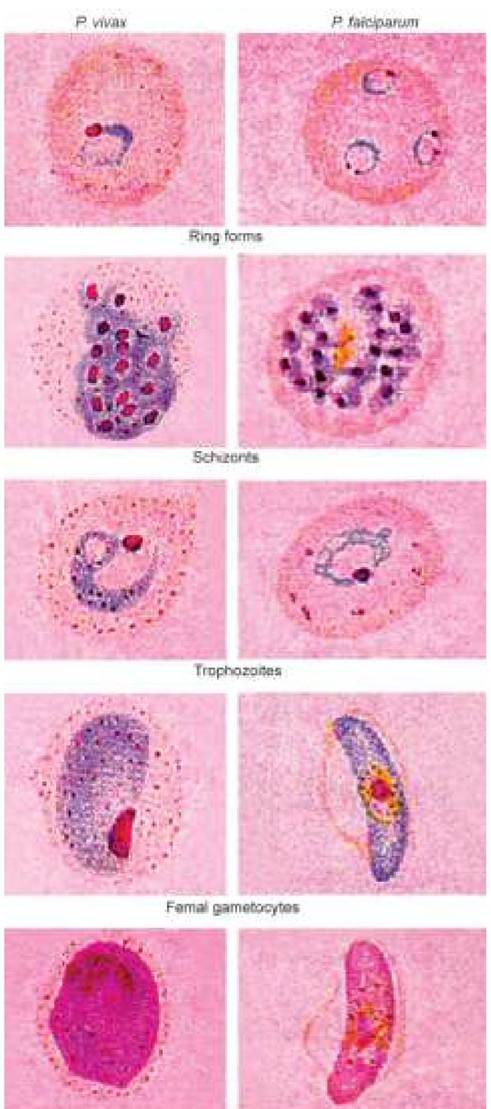
• Peripheral smear (PS): Demonstration of ring or trophozoite stage on PS is the gold standard for diagnosis of malaria, though possible in only 50-60% cases. Smear yield is higher if—(a) PS is made during acute febrile episode and before anti-malarial therapy, (b) it is prepared from bone-marrow or splenic-aspirate, (c) special staining techniques are used, and (d) multiple smears are examined. Single negative smear does not exclude malaria. Thick and thin smear is most commonly used laboratory tool for demonstration of various stages of parasite (Fig. 10.18) that involves preparation of two smears: (a) a thick smear that increases chances of parasite detection due to more RBC mass, and (b) a thin smear to identify the species (Pv or Pf). Commonly used staining procedures include Field's stain, JSB stain and Giemsa stain (Table 10.54).
The term parasite index denotes percentage of parasite-laden erythrocytes, used as a marker of the disease-severity as well as therapeutic response.
• Rapid diagnostic tests (RDTs), based on the detection of circulating parasite antigens, are useful to detect malarial infection when microscopy is not possible or delayed. However, these tests should not be used as replacement for microscopy. Among the available RDTs, some can detect only the Pf species (monovalent) while others can also identify Pv or other species (bivalent). Two commonly used RDTs are as follows:
Parasight-F test is a monovalent RDT, which detects histamine-rich protein (HRP-2) antigen of asexual Pf, with sensitivity of gt;90% in cases with parasite load of gt;100-500#8725;#956;l. However, it may be false-negative in very low parasitemia and false-positive in posttreatment cases as HRP-2 antigen may persist for up to 4 weeks after parasite clearance on treatment. This test cannot detect Pv infection.
Optimal test is a bivalent RDT that detects parasitic LDH enzyme, produced by all species. Sensitivity and specificity of optimal test is gt;95% in diagnosis of Pf as well as Pv malaria. It is capable to detect parasite load of as less as 50-100 parasites/ #956;l and becomes negative after successful treatment.
Sensitivity of RDT depends on the quality and storage conditions of the kit, species and load of the parasite and technique and care used during testing. RDTs may be used as a screening test, though a
UJe j?#947; divide;!zc#8730;!cl
Fig. 10.18: Peripheral smear in malaria—parasitic stages.
TABLE 10.54: Staining methods for PS-MP
Leishman's staining:
• Cover the smear with Leishman stain (1-2 min)
• Pour equal volume of buffer water (7-10 min)
• Wash with water and dry
Giemsa staining:
• Fix the smear with acetone-free methanol (1min)
• Cover with giemsa's stain (20 min)
• Wash with water and dry
negative RDT in a strongly suspected case should always be confirmed by microscopy. RDT may not differentiate between active infection and recent effectively treated infections and should not be used to monitor the response to therapy.
• Other diagnostic tests of limited utility, include- special staining techniques, antibody detection tests and molecular diagnostic tests. QBC test or Acridine- Orange staining involves fluorescent staining of parasitic nucleic acids. It is useful to detect very low parasitemia (~2-3#8725;#956;l), but species identification is difficult. Antibody detection tests are of little clinical significance in endemic regions due to past infection and molecular tests are confirmatory but not freely available. Other laboratory abnormalities, though not diagnostic, help in early detection of severe malaria and include severe anemia, thrombocytopenia and hypoglycemia.
Table 10.55 provides an overview of main epidemiological, clinical and laboratory differences between Pv and Pf malaria.
Management of malaria aims to: (a) cure the disease, (b) prevent relapses, (c) render the patient non-infective, and
(d) prevent the infection. It includes specific antimalarial therapy as well as supportive measures, e.g. antipyretics, fluid-electrolyte correction, adequate nutrition and treatment of complications.
TABLE 10.55: P. vivax vs P. falciparum malaria
| P. vivax | P. falciparum | |
| Life cycle | ||
| No. of Merozoites1 | bgcolor=white>lt;15,000gt;40,000 | |
| Affected RBCs | Young | Any |
| Parasite index | lt;5% | gt;10-30% |
| EE phase2 | Present | Absent |
| Gametocytes3 | 4-5th day | 10-2th day |
| Clinical features | ||
| Fever periodicity | 48 hours | Usually absent |
| Complications | Uncommon | Severe malaria |
| Relapse | No | Yes |
| Smear findings | ||
| RBC size | Enlarged | Normal |
| RBC stippling | Schuffner's dots4 | Maurer's spots5 |
| Ring stage/RBC | Large, 1-2 rings | Small, multiple |
| Schizont | Large, ameboid | Small, compact |
| Pigment | Golden haze | Dark brown |
| Gametocytes | Spherical | Cresent-shape |
| Response to treatment | ||
| Drug resistance | Rare | Common |
1Number of merozoites released from hepatic phase; 2exoerthro- cytic phase; 3day of gametocyte appearance; 4small, numerous, red dots; 5large, lt;20, red dots.
No single anti-malarial agent is effective against all stages of parasite. Currently available drugs may be divided into three groups:
a. Drugs acting on hepatic phase, which destroy the sporozoites, prevent hepatic schizogony or prevent erythrocyte invasion by merozoites, e.g. pyrimethamine, primaquine, proguanil. These drugs are used to prevent the disease after exposure, i.e. chemoprophylaxis or to prevent relapses, i.e. radical cure in Pv malaria.
b. Drugs acting on erythrocytic phase, which inhibit erythrocytic schizogony and rupture of infected RBCs. These drugs, e.g. chloroquine, quinine, mefloquine merely suppress the Pv infection due to limited action on exo- erythrocytic phase; but are curative for Pf infection with no exo-erythrocytic phase. A combination of drugs effective against both erythrocytic and hepatic phase must be used for complete clinical as well as radical cure in Pv malaria, e.g. chloroquine with primaquine.
c. Gametocidal drugs, which destroy gametes to prevent further transmission in new vectors, e.g. primaquine, mefloquine, etc. Chloroquine is not gametocidal.
d. Sporonticidal drugs prevent maturation of parasite within the mosquito to break transmission cycle, e.g. pyrimethamine, proguanil, etc.
e. Broad-spectrum antimalarial drugs, e.g. artemisinin derivatives, effective against all forms of erythrocytic stages and gametocytes (except mature forms). However, these drugs are ineffective against extra- erythrocytic forms, sporozoites and merozoites.
Artemisinin combination therapy (ACT) has revolutionized the treatment of falciparum malaria. It involves simultaneous use of two or more schizonticidal drugs with different mode of action. One of the partners in this combination should be an artemisinin derivative due to its high killing rate (reduces parasite load 10,000 fold versus 100-1000 fold per cycle with other drugs), lack of serious side effects, low level of resistance and rapid elimination of the drug, which ensures that the parasites are not exposed to sub-therapeutic levels. When combined with slowly-eliminated antimalarials, e.g. lumefantrine or sulfadoxinepyrimethamine (SP), artemisinin derivatives also protect against emergence of drug resistance by drastically reducing the number of parasites exposed to these long-acting drugs.
Five ACT combinations are approved by WHO for use in children-Artesunate+Sulfadoxine-Pyrimethamine (ASP), Artesunate+Amodiaquine (AA), Artesunate+mefloquine (AM), Artemether+Lumefantrine (AL) and Dihydro- artemisinin+Piperaquine (DHP).
WHO 2023 and National Vector Borne Diseases Control Programme (NVBDC) guidelines recommends that all fever cases with suspected malaria should be investigated for confirmation, preferably with microscopy or by RDT, before initiation of the treatment. Specific chemotherapy
in malaria depends on the species of parasite, prevalent pattern of drug-resistance as well as clinical status of patient and may be broadly divided into management of—(a) uncomplicated attack, (b) drug-resistant malaria, and (c) severe malaria.
a. Treatment of uncomplicated vivax malaria: Chloroquine continues to be the drug of choice in all cases of uncomplicated Pv malaria, followed Primaquine for 14 days to eliminate the exo-erythrocytic phase for radical cure (Table 10.56).
WHO 2023 recommends Chloroquine in 3 doseschedule (PO 10 mg/kg stat, 10 mg/kg after 24 hrs and 5 mg/kg after 48 hrs), preferable to the conventional four-dose schedule (PO 10 mg/kg stat than 5 mg/ kg at 6, 24 and 48 hrs), though total dose is same, i.e. 25 mg/kg. Dose should be repeated if patient vomits within 30 minutes.
In regions with chloroquine-resistant Pv, ACT containing Lumefantrine, mefloquine or Piperaquine (AL, AP or AM) is recommended for uncomplicated Pv malaria (WHO 2023).
Primaquine is contraindicated in infants, pregnancy, lactation and G6PD deficiency. G6PD estimation is advisable in all cases before primaquine therapy, if possible. While 14-day Primaquine therapy is recommended for radical cure, WHO 2023 also recommends additional option of PO Primaquine 0.5 mg/kg/day for 7 days for better compliance of shorter regimen.
G6PD deficient children may be given 0.75 mg/ kg of Primaquine once a week for 6 weeks instead of usual daily dose for 14 days.
b. Treatment of uncomplicated falciparum malaria: Considering the high frequency of Chloroquine and Pyrimethamine resistance in India, ACT is the treatment of choice for uncomplicated Pf malaria.
TABLE 10.56: Treatment of uncomplicated malaria
Of these, only two-ASP (for states other than northeastern states) and AL (for north-eastern states) are recommended in National Drug Policy for malaria (Table 10.56).
ASP is not recommended in north-eastern states due to high incidence of Pyrimethamine resistance, in newborns due to risk of competitive bilirubin displacement by SP leading to hyperbilirubinemia, and in HIV-infected children on Cotrimoxazole prophylaxis.
Author's note: Author prefers AL over ASP due to: (a) lack of liquid ASP formulations, and (b) risk of missing SP in ASP combinations, as it is provided as separate tablet.
In all cases of Pf malaria, ACT should be followed by single dose of Primaquine (0.75 mg/kg) to destroy the gametocyte and break the transmission cycle, except in infants lt;6 months. G6PD testing is not required (WHO 2023).
c. Treatment of mixed malaria is similar to that for pf malaria, except that primaquine has to be given as PO 0.25 mg/kg/day for 14 days, as for Pv malaria (Table 10.56).
d. Treatment of severe malaria is life-threatening and specific ant-malarial therapy in all cases including infants, should begin parenterally with any of the three drugs - artesunate, artemether or quinine for at Ieastfirst 24 hours, followed by switch-over to oral therapy as early as possible (Table 10.57).
While National Drug Policy lists Quinine, Artesunate and Artemether in the order of treatment of severe malaria, WHO 2023 recommendations favour Artesunate as the preferred choice, since it takes ~4 hours to achieve adequate quinine levels even after the loading dose. If artesunate is not available, artemether should be used in preference to quinine for severe malaria.
Children weighing lt;20 kg should receive a higher dose of artesunate (3 mg/kg per dose) than larger
TABLE 10.57: Treatment of severe malaria (Any one)
children and adults (2.4 mg/kg per dose) to ensure equivalent exposure to the drug.
Following initial parenteral therapy, PO Doxycycline (3.5 mg/kg OD in children gt;8 yrs) or PO Clindamycin (10 mg/kg BD in younger children lt; 8 yrs) for 7 days must be added to prevent development of resistance. However, WHO 2023 recommends switch-over to oral ACT for 3 days due to poor adherence for 7-day treatment regimens using doxycycline or clindamycin.
Intensive care with supportive therapy is also essential in these cases, including:
• Restoration of fluid and electrolyte balance, with early correction of metabolic acidosis. However, overhydration must be avoided to prevent pulmonary edema.
• Regular monitoring of blood sugar for early detection and treatment of hypoglycemia.
• Correction of anemia with transfusions or preferably partial exchange transfusion, which also helps to reduce parasite load.
• Control of seizures with anticonvulsants, e.g. phenobarbitone or diazepam.
• Organ-specific supportive management, as required.
• Treatment of cerebral malaria, the commonest form of severe malaria is discussed in Ch 18.12.6.
Treatment failure in malaria is defined as failure of the fever and/or parasitemia to resolve or recur after treatment within 28 days, further classified as early treatment failure (no response in 3 days) or late treatment failure (4-28 days). Absence of parasitemia on day 28 is considered as adequate clinical and parasitological response (ACPR). All cases of treatment failure are not due to drug resistance and many may represent recrudescence or relapse due to inadequate treatment or re-infection.
Management of these cases, as per current WHO recommendation (2023) is as follows:
• Recurrence of fever or parasitemia within 28 days is more likely due to recrudescence of infection and must be treated second-line treatment, i.e. an alternative ACT known to be effective in the region.
• Recurrence of fever and parasitaemia after 28 days of treatment may be due to either recrudescence, relapse or re-infection. Distinction can be made only by PCR genotyping of parasites from the initial and the recurrent infections. Since PCR is not routinely used in patient management, all presumed treatment failures after 4 weeks of initial treatment should be considered new infections and treated with the first-line ACT. However, reuse of mefloquine within 60 days of first treatment is not recommended due to increased risk for neuropsychiatric reactions.
Prevention: Malaria control strategies in India have been revised periodically, to meet the changing epidemiology, occurrence of outbreaks, drug-resistance and insecticide resistance in vectors.
Malaria vaccines: More than thirty vaccines against Pf malaria are at pre-clinical and clinical stages of evaluation, acting on different stages of the parasite. However, RTS, S (Mosquirix®) is the only vaccine licensed on pilot basis in three sub-Saharan African countries - Ghana, Kenya and Malawi, and has shown significant reduction in prevalence as well as severity of falciparum malaria (Ch 9.2.4). An indigenous malaria vaccine, developed by Serum Institute of India, Pune has also been approved recently and, is expected to available soon.
National Vector Borne Diseases Control
Programme (Malaria)
Malaria control strategies in India date back to 1953 with launching of National Malaria Control Programme, which has been subsequently modified many times, presently being the part of National Vector-borne Disease Control Programme (NVBDCP), since 2002. Important components of this program are as follows:
a. Early diagnosis and management of malaria cases to reduce the reservoir by:
- Passive surveillance, i.e. examination of peripheral smear in all febrile cases, covering at least 10% of total population, annually.
- Standardized protocols for diagnosis, including use of rapid diagnostic tests in areas where microscopy facility is not available.
- Standardized protocols for treatment, including use of artemisinin-combination therapy in falciparum malaria due to high frequency of chloroquine- resistance.
- Radical treatment of confirmed vivax malaria for 14 days.
- Presumptive anti-malarial therapy is no longer recommended except in cases from endemic regions with high suspicion of malaria, provided microscopy result is not available within 24 hours and bivalent RDT is not possible. In such cases, full 3-days course of chloroquine is recommended without Primaquine, which should be used only in confirmed cases. Treatment must be modified after smear or RDT results.
b. Chemoprophylaxis is indicated only selective groups, e.g. military personals, travelling to high Pf endemic areas, along with other personal protection measures, e.g. insecticide-treated nets.
- Short-term chemoprophylaxis (lt;6 weeks) involves PO Doxycycline 1.5 mg/kg OD from 2 days before to 4 weeks after the exposure. It is contraindicated in children lt;8 years or pregnant women.
- Longer chemoprophylaxis (gt;6 weeks) is advised only in adults (not children) with PO Mefloquine 250 mg/week from 2 days before to 4 weeks after the exposure. It is contraindicated in individuals with history of convulsions, neuropsychiatric problems and cardiac conditions.
c. Vector control to reduce the transmission, by:
- Anti-adult mosquito measures, e.g. residual spraying/ fogging, with DDT, malathion, fenitrothion, etc.
- Anti-larval measures, e.g. source reduction (reducing breeding sites), use of chemical larvicidals (oil, temphos) or biological agents, e.g. fishes.
- Personal protection measures, e.g. nets, repellents, etc.
d. Information, education and communication (IEC) campaign is intensified during pre-monsoon season, i.e. June (declared as anti-malaria month).
e. Ancillary activities, e.g. research, training, etc.
National Framework of Malaria
Elimination (2016-2030)
In line with the WHO Global Technical Strategy for Malaria 2016-2030, National Framework for Malaria Elimination 2016-2030 outlines India's strategy for elimination of the disease by 2030 with well-defined goals, strategies, targets and timelines. It aims to: (a) eliminate malaria (zero indigenous cases) throughout the entire country by 2030, (b) maintain malaria-free status in areas where malaria transmission has been interrupted, and (c) prevent re-introduction of malaria.
10.34
More on the topic 10.33 MALARIA MYCOPLASMA INFECTIONS:
- Hemotropic Mycoplasma Infections
- MYCOPLASMA INFECTIONS OF AQUATIC MAMMALS
- CLINICAL SPECTRUM
- Aspiration Pneumonia
- Genital Warts
- Aetiologies of Illness
- Malaria
- OTHER MYCOPLASMA INFECTIONS
- Malaria Education
- Mycoplasma spp. Infections