NUTRITIONAL, METABOLIC AND TOXIC DISORDERS
Cystic Mastitis
Sterile fluctuant cysts with swollen teats may involve any mammary gland in rabbits of both sexes and all ages. These changes wax and wane with the hormone status, and disappear during estrus, pregnancy, pseudopregnancy, or lactation and reappear in the resting postlactation period.
In virgin females, they disappear with first estrus. They are purported to progress to neoplasia. Ovariohysterectomy has been noted to ameliorate the disease. Microscopically, ducts are dilated and lined by flattened or hyperplastic epithelium and in some, epithelium is lost with associated inflammation. In 1 report, these changes were noted in aged nulliparous New Zealand White rabbits in association with prolactin-secreting pituitary adenomas.Pregnancy Toxemia
Pregnancy toxemia is a poorly characterized condition that occurs in does, usually during the last week of pregnancy or the immediate postpartum period. Obesity and fasting are important predisposing factors. The disease is characterized by low morbidity and high mortality. Multiparous does are especially at risk, and metabolic toxemia may also occur on occasion in obese, “stressed,” nonpregnant rabbits. Obesity, hereditary predisposition, impaired blood flow to the uterus, and pituitary dysfunction are factors implicated in this disease. There is 1 report of pregnancy toxemia and concurrent pancreatitis in a New Zealand White doe. Clinical manifestations of the disease are variable and may include incoordination, abortions, and coma. Most does fail to respond to treatment. In the typical case of pregnancy toxemia, mobilization of fat deposits for energy results in metabolic acidosis and ketosis, depression, and death. At necropsy, animals are usually obese, with marked fatty infiltration of the liver and adrenal glands.
Hypocalcemic Tetany in Lactating Does
There is a marked drain on serum calcium levels in does during the first month of lactation that can result in hypocalcemia and tetany.
In 1 report in which rabbits were fed a commercial diet and hay, 6 of 31 Fauve de Bourgogne does were found lying on their side, and had signs that included ear flapping, jerking of posterior limbs, and muscle tremors. Plasma calcium levels were measured in affected rabbits, and found to be 5.8 ± 0.4 mg/dl, whereas plasma calcium in nonlactating control does was 13.8 ± 0.2 mg/dl.Hypercalcemic Arteriosclerosis
As noted previously, rabbits absorb calcium in proportion to levels in their diet, and depend upon renal excretion for regulation of serum calcium levels. They are, therefore, vulnerable to hypercalcemia when confronted with severe renal disease (chronic renal disease, lymphosarcoma, etc.), which can be exacerbated by secondary hyperparathyroidism and excess dietary vitamin D. Hypercalcemia results in metastatic mineralization of blood vessels (Fig. 6.92) and other tissues, including pulmonary interstitium, and kidneys (neph- rocalcinosis). Arterial lesions include mineral deposition in the tunica media, with macrophage infiltration and smooth muscle degeneration. The early mineral composition of aortic lesions was found to contain calcium phosphate, dicalcium phosphate dehydrate, and octacalcium phosphate, with later development of
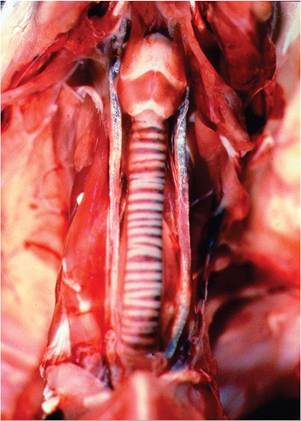
FIG. 6.92. Metastatic mineralization of the carotid arteries in a rabbit with hypercalcemia secondary to chronic renal disease.
hydroxyapatite crystals. In an atherogenesis study, rabbits were shown to develop dystrophic mineralization of atheromatous lesions, without disturbing calcium and phosphorous homeostasis, or mineralization of other tissues.
Nutritional Secondary Hyperparathyroidism
Chronic nutritional hypocalcemia with secondary hyperparathyroidism and decreased bone mass has been reported in rabbits fed a diet deficient in calcium. It was rapidly reversible with appropriate calcium supplementation. Dental disorders, similar to vitamin D deficiency, may also occur.
Atherosclerosis/Hypercholesterolemia
Rabbits are highly susceptible to hypercholesterolemia when fed high-cholesterol diets. Rabbits are unable to increase excretion of sterols, resulting in an enhanced hepatic export of cholesteryl ester-rich lipoproteins into the bloodstream. Hypercholesterolemia, in association with LDL and beta-VDL, is induced within a few days of feeding a high-cholesterol diet. Arterial plaques, ranging from fatty streaks to atheromas, arise in the aorta and coronary arteries. The aortic arch and thoracic aorta are predisposed at lower doses, whereas the entire aorta may be involved with higher dietary doses. Microscopic evidence of myocardial infarction is common. New Zealand White rabbits are the most frequently used breed of rabbit, but long-term experiments are hampered because of cholesterol-induced hepatopathy, which includes severe hepatic lipidosis (Fig. 6.93) and hepatocellular necrosis, with bile stasis and icterus. A number of inbred and transgenic rabbits have been developed for atherosclerosis research. Watanabe heritable hyperlipidemic (WHHL) rabbits have been particularly well studied.

FIG. 6.93. Hepatic lipidosis in a New Zealand White rabbit fed a high-cholesterol diet. Rabbits are unable to increase excretion of sterols in the bile in response to high cholesterol in the diet, resulting in hypercholesterolemia, hepatic lipidosis, and icterus.
Homozygous WHHL rabbits have a genetic deficiency of LDL receptors, and develop atherosclerotic arterial plaques and xanthomatous lesions in the digital joints, pia, and eye. WHHL rabbits develop atherosclerosis without feeding high-cholesterol diets.
Xanthomatosis/Hypercholesterolemia
Because of the prevalence of research on atherosclerosis using rabbits, including outbred New Zealand White rabbits, hypercholesterolemic rabbits may develop a number of nonvascular lesions of note.
Dermal xanthomas have been shown to arise in the upper dermis, which was infiltrated with lipid-laden macrophages, as well as vascular pericytes throughout the dermis. Infiltration of lipid-laden macrophages or lipidosis arises in many tissues, including muscle, heart, lung, choroid plexus, kidney, gastrointestinal tract, and endocrine organs. Lipid keratopathy has been frequently reported in rabbits, including rabbits fed a commercial diet. Typically, the corneoscleral junction may be irregularly infiltrated with yellowish-white granular opacities, representing lipid-laden xanthoma cells. Xanthoma cells may also commonly infiltrate other regions of the eye. They can be seen grossly involving the iris (Fig. 6.94), and microscopically involving ciliary body, choroids, and sclera (Fig. 6.95). In 1 report of a rabbit fed a high-cholesterol diet, lipid-laden macrophages were not only observed in the eye, but also the dermis, lung, lymphoid tissue, and choroid plexus of the brain.Vitamin A Toxicity or Deficiency
The clinical manifestations of vitamin A toxicity or deficiency are similar in domestic rabbits to those of other species, and are characterized by poor conception rates, congenital anomalies, fetal resorptions, abortion, and weak, thin kits. Congenital defects associated with hypervitaminosis A include microencephaly, hydrocephalus, and cleft palate. Rabbits are unique in that they can convert 100% of dietary beta-carotene into retinol. A case of hyperostotic polyarthropathy, presumptively diagnosed as hypervitaminosis A, has been reported in a pet rabbit that was chronically fed a diet of carrots.

FIG. 6.94. Iridial xanthomatosis in a New Zealand White rabbit fed a high-cholesterol diet.
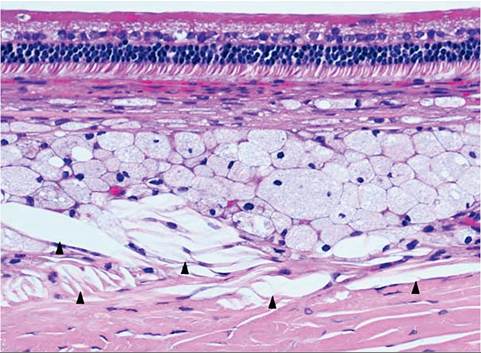
FIG. 6.95. Xanthoma cells and cholesterol clefts (arrow heads) in periocular tissue of a rabbit with hypercholesterolemia.
(Source: Kouchi et al. 2006. Reproduced with permission from Wiley.)Vitamin D Toxicity or Deficiency
The requirement for vitamin D is lower in rabbits compared to other mammals, and they are therefore prone to vitamin D intoxication. The problem usually arises when rabbits are fed an improperly formulated diet. Affected rabbits are anorectic with weight loss. They manifest muscle weakness and paresis. Histologic changes include medial degeneration and mineralization of major arteries. Mineralization of the glomerular tufts, basement membranes, and tubules of the kidney may also occur. In the long bones, there is deposition of basophilic material on the periosteal and endosteal surfaces, medullary trabeculae, and Haversian systems. In contrast, vitamin D deficiency presents as anemia, immunodeficiency, and osteomalacia. Dental disorders may also arise, with overgrowth and ridging of the incisor teeth and distorted growth of the premolar and molar teeth.
Vitamin E Deficiency
There are several reports of nutritional muscular dystrophy due to vitamin E deficiency. In addition to stiffness and muscle weakness, neonatal mortality and infertility are manifestations of vitamin E deficiency in domestic rabbits. At necropsy, pale mineralized streaks may be present in musculature, such as the diaphragm, paravertebral regions, and hind limbs. Typical changes seen microscopically are hyaline degeneration of affected myofibers and clumping and mineralization of the sarcoplasm. Macrophages may be present in reactive areas. Collapse of sarcolemmal sheaths and interstitial fibrosis frequently occur in lesions of some duration.
Copper Toxicosis
Copper sulfate is often added to rabbit feed as a supplement. Copper is generally well tolerated, but rabbits are considered to be sensitive to copper. A number of cases of copper toxicosis have been reported in domestic rabbits. Acute toxicity was associated with hemolytic anemia with intravascular hemolysis, erythrophagocy- tosis in the spleen, hepatic centrilobular to midzonal necrosis, and hematuria with tubular casts.
Periportal fibrosis and biliary hyperplasia have also been noted. Hepatocytes and Kupffer cells contained blue-green cytoplasmic granules that stained positive with rhodanine stain. In 1 outbreak, shipping stress and dietary change appeared to precipitate disease.Fluoride Toxicosis: Osteofluorosis
Moderate to severe osseous proliferations of the extremities (Fig. 6.96) and mandibles were observed among growing rabbits in 2 European rabbitries. Bones had periosteal and endosteal hyperostosis. In addition, affected rabbits had marked proliferation of gastric and duodenal mucosa, but it is unclear if the gastrointestinal lesions were related. Bone ash analysis revealed high levels of fluoride reaching over 20 times the normal level. The source of the fluoride was pelleted feed produced by 2 different feed mills. Other outbreaks of osteofluorosis have been reported in rabbits from Mexico.
Lead Toxicosis
With the propensity of rabbits to chew foreign items including painted objects, it is not surprising that lead toxicosis is common among “free-ranging” pet rabbits, but can also occur in commercial and laboratory rabbits in cage environments with lead components (solder).

FIG. 6.96. Hyperostosis of the tarsus and metatarsus of a rabbit with chronic fluoride toxicosis. (Source: Bock et al. 2007. Reproduced with permission from SAGE Publications.)
Clinical signs include anorexia, tremors, seizures, torticollis, blindness, and ataxia. In fatal cases of lead toxicosis, myocardial degeneration, multifocal hepatic necrosis, renal tubular degeneration, and hemoglobin casts in renal tubules are microscopic findings. Features of anemia include reticulocytosis, nucleated erythrocytes, hypo- chromasia, basophilic stippling, poikilocytosis, and anisocytosis. Chronically affected rabbits may be immunosuppressed. Diagnosis is confirmed with blood lead concentrations. Toxicosis is considered positive with blood levels greater than 30 pg/dl, but lower levels may be considered abnormal in chronic toxicosis. Chronic toxicosis is also reported to be associated with gastrointestinal stasis or diarrhea. In cases diagnosed antemortem, removal of all lead from the gastrointestinal tract is recommended prior to the administration of chelating agents, since chelation will enhance the absorption of any lead present in the gastrointestinal tract.
Aflatoxicosis
Aflatoxicosis was reported in an incident involving a large number of Angora rabbitries in India. Affected rabbits were anorectic, lost weight, and became jaundiced within 3-4 days of disease onset. Mortality was highest in juvenile rabbits. Livers were congested, icteric, and gall bladders were distended with inspissated bile. Microscopic findings featured hepatocellular degeneration, periportal fibrosis, and regenerative foci. The toxin was identified as aflatoxin B1 contamination of feed. Coagulation defects develop during B1 aflatoxicosis in the rabbit, with diminished synthesis of coagulation factors, or in the case of severe hepatic necrosis, intravascular coagulation, and consumption of coagulation factors take place. Among various species, rabbits are among the most highly sensitive to aflatoxin B1.
Poisonous Plant Toxicity
Through their innate curiosity or contamination of pelleted feed or hay, rabbits are subject to inadvertent toxicity upon ingestion of any one of a very large list of common toxic plants that reside out of doors or as houseplants. The list is far too extensive to cover, and the reader is referred to various rabbit fancier Web sites for access to further information.
Drug Toxicoses
In-depth coverage of suitable drugs for use in rabbits and side effects that may be encountered can be found in Textbook of Rabbit Medicine by Molly Varga and in a review entitled Clinical Toxicoses of Domestic Rabbits by Matthew Johnston. A few adverse effects of commonly used drugs are listed below.
Cardiomyopathy Associated with Ketamine/ Xylazine Administration
Multifocal myocardial degeneration with interstitial fibrosis has been observed in Dutch Belted rabbits following the administration of a ketamine/xylazine combination. A similar effect was found in New Zealand White rabbits given ketamine with the alpha2 agonist detomidine or detomidine alone. This change is attributed to ischemia secondary to vasoconstriction with reduction in coronary blood flow, with subsequent myocardial degeneration and fibrosis. Collateral circulation in the myocardium is limited in this species. In lesions of recent onset, there is degeneration of myofibers with mononuclear and polymorphonuclear leukocytic infiltration. In lesions of some duration, there is loss of myofibers and marked interstitial fibrosis. Borderline vitamin E deficiency could also contribute to the development of the myocardial lesions.
Fluoroquinolone Arthropathy
Baytril (enrofloxacin) is a safe and efficacious fluoroqui- nilone antibiotic for use in rabbits, but arthropathy is a notable side effect that has been documented in juvenile New Zealand White rabbits. The arthropathy features development of vesicular lesions in the articular cartilage of large weight-bearing joints.
Ionophore Toxicity
Ionophore drugs are commonly used as coccidiostats in rabbit feed. Outbreaks of narasin poisoning with high mortality have occurred when rabbits were fed a pelleted ration to which poultry ration premix was added. Rabbits became anorectic, weak, and had impaired walking, diarrhea, respiratory distress, and opisthotonus. Microscopic findings included myofiber necrosis and regeneration in skeletal muscles, with milder changes in myocardium. Some of the drugs used for poultry may not work as well in rabbits.
Telazol Nephrotoxicity
The anesthetic Telazol is used as an intramuscular anesthetic in a variety of species. Low (32 mg/kg; recommended dose) to high doses (64 mg/kg) in rabbits resulted in elevated blood urea nitrogen at 4 days after administration. Necropsy revealed marked multifocal nephrosis and nephrocalcinosis in both dose groups, but most severe in the high-dose group.
Antibiotic “Toxicity”
A number of antibiotics, including clindamycin, erythromycin, and oral beta-lactam antibiotics are associated with induction of enteric dysbiosis and Clostridial enterotoxemia (see “Clostridial Diseases”).
BIBLIOGRAPHY FOR NUTRITIONAL, METABOLIC, AND TOXIC DISORDERS
General Reference for Nutritional, Toxic, and Metabolic Diseases
Varga, M. (2013) Textbook of Rabbit Medicine, 2nd edn. Elsevier.
Cystic Mastitis
Atherton, J., Griffiths, L., & Williams, A. (1999) Cystic mastitis in the female rabbit. Veterinary Record 145:648.
Fifer, C.L. (1934) The breast. I. Lesions in rabbits resembling chronic cystic mastitis. Archives of Surgery 29:555-559.
Hughes, J.E., Chapman, W.L., & Prasse, K.W. (1981) Cystic mammary disease in rabbits. Journal of the American Veterinary Medical Association 178:138-139.
Lipman, N.S., Zhao, Z.B., Andrutis, K.A., Hurley, R.J., Fox, J.G., & White, H.J. (1994) Prolactin-secreting pituitary adenomas with mammary dysplasia in New Zealand White rabbits. Laboratory Animal Science 44:114-120.
Pregnancy Toxemia
Greene, H.S.N. (1937) Toxemia of pregnancy in the rabbit: clinical manifestations and pathology. Journal of Experimental Medicine 65:809-832.
Hypocalcemic Tetany in Lactating Does
Barlet, J.-P. (1980) Plasma calcium, inorganic phosphorus and magnesium levels in pregnant and lactating does. Reproduction Nutrition Development 20:647-651.
Hypercalcemic Arteriosclerosis
Ngatia, T.A., Mugera, G.M., Njiro, S.M., Kuria, J.K.N., & Carles, A.B. (1989) Arteriosclerosis and related lesions in rabbits. Journal of Comparative Pathology 101:279-286.
Rokita, E., Cichocki, T., Divoux, S., Gonsior, B., Hofert, M., Jarczyk, L., & Strzalkowski, A. (1992) Calcification of the aortic wall in hypercalcemic rabbits. Experimental and Toxicologic Pathology 44:310-316.
Rokita, E., Cichocki, T., Heck, D., Jarczyk, L., & Strzalkowski, A. (1991) Calcification of aortic wall in cholesterol-fed rabbits. Atherosclerosis 87:183-193.
Shell, L.G. & Saunders, G. (1989) Arteriosclerosis in a rabbit. Journal of the American Veterinary Medical Association 194:679-680.
Nutritional Secondary Hyperparathyroidism
Bas, S., Bas, A., Lopez, I., Estepa, J.C., Rodriguez, M., & Aguilera- Tejero, E. (2005) Nutritional secondary hyperparathyroidism in rabbits. Domestic Animal Endocrinology 28:380-390.
Harcourt-Brown, F.M. (1996) Calcium deficiency, diet and dental disease in pet rabbits. Veterinary Record 139:567-571.
Mehorotra, M,. Gupta, S.K., Kumar, K., Awasthi, P.K. Dubey, M., Pandey, C.M., & Godbole, M.M. (2006) Calcium deficiency- induced secondary hyperparathyroidism and osteopenia are rapidly reversible with calcium supplementation in growing rabbit pups. British Journal of Nutrition 95:582-590.
Atherosclerosis/Hypercholesterolemia
Aliev, G. & Burnstock, G. (1998) Watanabe rabbits with heritable hypercholesterolemia: a model of atherosclerosis. Histology and Histopathology 13:797-817.
Bocan, T.M., Mueller, S.B., Mazur, M.J., Uhlendorf, P.D., Brown, E.Q., & Kieft, K.A. (1993) The relationship between the degree of dietary-induced hypercholesterolemia in the rabbit and atherosclerotic lesion formation. Atherosclerosis 102:9-22.
Kolodgie, F.D., Katocs, A.S., Jr, Largis, E.E., Wrenn, S.M., Cornhill, L.F., Herderick, E.E., Lee, S.J., & Virmami, R. (1996) Hypercholesterolemia in the rabbit induced by feeding graded amounts of low-level cholesterol. Arteriosclerosis, Thrombosis, and Vascular Biology 16:1454-1464.
Xanthomatosis/Hypercholesterolemia
Fallon, M.T., Reinhard, M.K., DaRif, C.A., & Schoeb, T.R. (1988) Diagnostic exercise: eye lesions in a rabbit. Laboratory Animal Science 38:612-613.
Garibaldi, B.A. & Pequet Goad, M.E. (1988) Lipid keratopathy in the Watanabe (WHHL) rabbit. Veterinary Pathology 25:173-174.
Kouchi, M., Ueda, Y., Horie, H., & Tanaka, K. (2006) Ocular lesions in Watanabe heritable hyperlipidemic rabbits. Veterinary Ophthalmology 9:145-148.
Prior, J.T., Kurtz, D.M., & Ziegler, D.D. (1961) The hypercholester- olemic rabbit: an aid to understanding arteriosclerosis in man? Archives of Pathology 71:672-684.
Roth, S.I., Stock, L., Siel, J.M., Mendelsohn, A., Reddy, C., Preskill, D.G., & Ghosh, S. (1988) Pathogenesis of experimental lipid keratopathy: an ultrastructural study of an animal model system. Investigative Ophthalmology and Visual Science 29:1544-1551.
Sebesteny, A., Sheraidah, G.A.K., Trevan, D.J., Alexander, R.A., & Ahmed, A.I. (1985) Lipid keratopathy and atheromatosis in an SPF laboratory rabbit colony attributable to diet. Laboratory Animals 19:180-188.
Vitamin Toxicity/Deficiency
DiGiacomo, R.F., Deeb, B.J., & Anderson, R.J. (1992) Hypervitamin- osis A and reproductive disorders in rabbits. Laboratory Animal Science 42:250-254.
Frater, J. (2001) Hyperostotic polyarthropathy in a rabbit: suspected case of chronic hypervitaminosis A from a diet of carrots. Australian Veterinary Journal 79:608-611.
Ringler, D.H. & Abrams, G.D. (1970) Nutritional muscular dystrophy and neonatal mortality in a rabbit breeding colony. Journal of the American Veterinary Medical Association 157:1928-1934.
Ringler, D.H. & Abrams, G.D. (1971) Laboratory diagnosis of vitamin E deficiency in rabbits fed a faulty commercial ration. Laboratory Animal Science 21:383-388.
St Claire, M.B., Kennett, M.J., & Besch-Williford, C.L. (2004) Vitamin A toxicity and vitamin E deficiency in a rabbit colony. Contemporary Topics in Laboratory Animal Science 43:26-30.
Stevenson, R.G., Palmer, N.C., & Finley, G.G. (1976) Hypervita- minosis D in rabbits. Canadian Veterinary Journal 17:54-57.
Yamimi, B. & Stein, S. (1989) Abortion, stillbirth, neonatal death, and nutritional myodegeneration in a rabbit breeding colony. Journal of the American Veterinary Medical Association 194:561-562.
Zimmerman, T.E., Giddens, W.E., Jr, DiGiacomo, R.F., & Ladiges, W.C. (1990) Soft tissue mineralization in rabbits fed a diet containing excess vitamin D. Laboratory Animal Science 40:212-214.
Copper, Fluoride, and Lead Toxicity
Bock, P., Peters, M., Bago, Z., Wolf, P., Thiele, A., & Baumgartner, W. (2007) Spontaneously occurring alimentary osteofluorosis associated with proliferative gastroduodenopathy in rabbits. Veterinary Pathology 44:703-706.
Cooper, G.L., Bickford, A.A., Charlton, B.R., Galey, F.D., Willoughby, D.H., & Grobner, M.A. (1996) Copper poisoning in rabbits associated with acute intravascular hemolysis. Journal of Veterinary Diagnostic Investigation 8:394-396.
DeCubellis, J. & Graham, J. (2013) Gastrointestinal disease in guinea pigs and rabbits. Veterinary Clinics of North America Exotic Animal Practice 16:421-435.
Gerken, D.F. & Swartout, M.S. (1986) Blood lead concentrations in rabbits. American Journal of Veterinary Research 47:2674-2675.
Hood, S., Kelly, J., McBurney, S., & Burton, S. (1997) Lead toxicosis in 2 dwarf rabbits. Canadian Veterinary Journal 38:721-722.
Johnston, M.S. (2008) Clinical toxicoses of domestic rabbits. Veterinary Clinics of North America Exotic Animal Practice 11:315-326.
Koller, L.D. (1973) Immunosuppression produced by lead, cadmium and mercury. American Journal of Veterinary Research 34:1457-1458.
Ramirez, C.J., Kim, D.Y., Hanks, B.C., & Evans, T.J. (2013) Copper toxicosis in New Zealand White rabbits (Oryctolagus cuniculus). Veterinary Pathology 50:1135-1138.
Swartout, M.S. & Gerken, D.F. (1987) Lead-induced toxicosis in two domestic rabbits. Journal of the American Veterinary Medical Association 191:717-719.
Vinlove, M.P., Britt, J., & Comelium, J. (1992) Copper toxicity in a rabbit. Laboratory Animal Science 42:614-615.
Aflatoxicosis
Baker, D.C. & Green, R.A. (1987) Coagulation defects of aflatoxin intoxicated rabbits. Veterinary Pathology 24:62-70.
Krishna, L., Dawra, R.K., Vaid, J., & Gupta, V.K. (1991) An outbreak of aflatoxicosis in Angora rabbits. Veterinary and Human Toxicology 33:159-161.
Makkar, H.P.S. & Singh, B. (1991) Aflatoxicosis in rabbits. Journal of Applied Rabbit Research 14:218-221.
Drug Toxicoses
Brammer, D.W., Doerning, B.J., Chrisp, C.E., & Rush, H.G. (1991) Anesthetic and nephrotoxic effects of Telazol in New Zealand White rabbits. Laboratory Animal Science 41:432-435.
Hurley, R.J., Marini, R.P., Avison, D.L., Murphy, J.C., Olin, J.M., & Lipton, N.S. (1994) Evaluation of detomidine anesthetic combinations in the rabbit. Laboratory Animal Science 44:472-478.
Marini, R.P., Li, X., Harpster, N.K., & Dangler, C. (1999) Cardiovascular pathology possibly associated with ketamine/xylazine anesthesia in Dutch Belted rabbits. Laboratory Animal Science 49:153-160.
Salles, M.S., Lombardo de Barros, C.S., & Barros, S.S. (1994) Ionophore antibiotic (narasin) poisoning in rabbits. Veterinary and Human Toxicology 36:437-444.
Sharpnack, D.D., Mastin, J.P., Childress, C.P., & Henningsen, G.M. (1994) Quninolone arthropathy in juvenile New Zealand White rabbits. Laboratory Animal Science 44:436-442.
More on the topic NUTRITIONAL, METABOLIC AND TOXIC DISORDERS:
- NUTRITIONAL, METABOLIC, AND TOXIC DISORDERS
- NUTRITIONAL AND METABOLIC DISORDERS
- METABOLIC DISORDERS IN NEWBORN
- Nutritional Disorders
- Metabolic Disorders
- Chapter 6 METABOLIC DISORDERS
- GENETIC, METABOLIC, AND OTHER DISORDERS
- Antiretroviral Therapy and Metabolic Disorders
- A metabolic disease, or metabolic disorder, is the name given to a group of illnesses in dairy cows which are caused by an over-exertion of their normal metabolism.
- Toxic Alcohols
- Toxic Shock Syndrome