A metabolic disease, or metabolic disorder, is the name given to a group of illnesses in dairy cows which are caused by an over-exertion of their normal metabolism.
These diseases are generally seen during early lactation, when milk yields are at a peak, and they are due to an imbalance between the input of the cow’s food compared with her output in terms of maintenance, pregnancy and lactation.
As such they are sometimes referred to as production diseases. The main metabolic disorders are:• milk fever
• hypomagnesaemia
• acetonaemia
• fatty liver syndrome
• rumen acidosis
Rumen acidosis is slightly different from the other metabolic diseases because it is primarily a disorder of the rumen with secondary effects on the metabolism of the cow.
The Nature of Metabolic Disease
For a better understanding of the mechanisms of a production disease, take the analogy of a cold-water header tank in the roof of a domestic house, as shown in Figure 6.1. Water enters the tank via the input pipe and when it reaches a certain level its flow is shut off by a ball-valve. There will be various uses for the water; for example, there will be one feed to the kitchen, another to the bathroom and a third to the heating plant.
When the ball-valve is open, water will enter the tank at a constant rate and the level of water in the tank will be determined by the rates of outflow; that is, to the kitchen, bathroom and heater. If the system was badly designed, it is possible that output will exceed input, in which case the tank runs dry and various problems occur (e.g. air-blocks, or the heating plant boils).
A dairy cow may be looked at in a similar way. Although she may have several feeds during the day, the rate of flow of nutrients from the rumen into her bloodstream (the input) is virtually constant. These nutrients, or metabolites as they are correctly called, are used for a variety of purposes (the output). Their main functions are for maintenance (for movement, warmth and tissue respiration), pregnancy (and the adult cow should spend about 75% of her life pregnant) and,
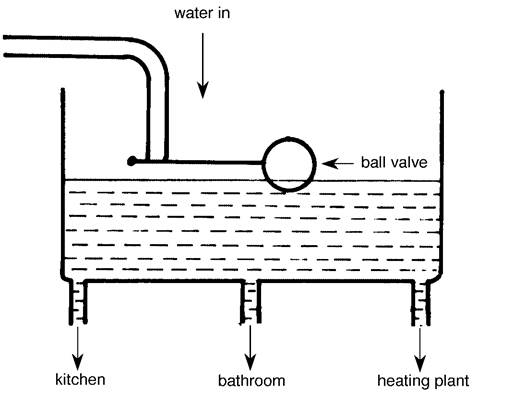
Figure 6.1.
The cold-water header tank analogy - factors affecting the level of water in the tank.most important of all, milk production. For a dairy cow therefore the water tank principle can be rewritten as in Figure 6.2.
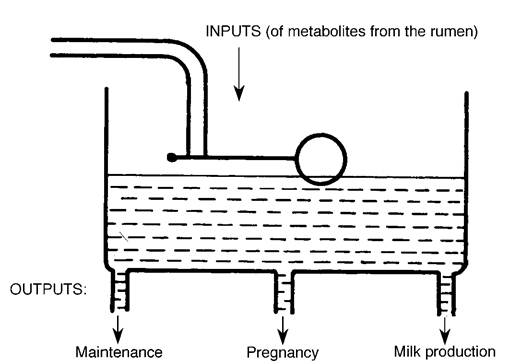
For a constant input of metabolites from the rumen, the level of ‘water’ in the tank (or in this analogy, the level of the metabolites circulating in the bloodstream) is governed by the overall rate of output. If output increases without any corresponding rise in input, the level of metabolites will fall until the tank is empty and this is when metabolic disorders occur.
Metabolic Profile Tests
We can take blood samples to measure
the level of metabolites in the Figure 6.2. The water tank analogy used to explain the concept circulation and this is known as a of production disease and metabolic profiles.
metabolic profile test. The metabolic
profile is an extremely useful technique for monitoring the nutritional and health status of dairy cows in that it tries to identify problems before they are seen as overt disease. The test measures the ‘balance’ between input, in terms of food, and output, based on the cow’s requirements of nutrients for maintenance, pregnancy and lactation. Metabolic profiles are only an aid in the investigation of production diseases however, and great care is needed both with the selection of cows to be blood sampled and in the interpretation of results. Even so, they can give very useful information on herd problems, such as:
• unsatisfactory milk production or milk quality
• high incidence of metabolic diseases
• assessment of dietary energy and protein status
• investigation of suboptimal fertility
• mineral and trace element deficiencies
One of the commonest mistakes made with metabolic profiles is that the wrong animals are sampled. For example take a herd where production is disappointing, the problem being that some cows fail to reach peak yield while others drop off rapidly from an early peak.
Cows which have already fallen in yield have of course decreased their production to match the food intake being received, that is their output has dropped to balance input. These would be the wrong animals to blood sample. It can be seen in Figure 6.2 that if their milk yield has fallen to match the food intake being received, then their blood levels will have returned to normal - and the initial cause of the production failure will no longer be apparent. If you are trying to assess the nutritional status of your herd, therefore, it is essential to choose normal cows with average to good production; otherwise the cause of the problem may be missed. Do not choose the one 60 litre cow in your herd - we know she is being underfed!Normally cows in the early lactation stage are sampled, for example at around four to eight weeks after calving. This is certainly the best group to examine when energy and protein balance are being checked, and there is also the advantage that cows at this stage of lactation are approaching the service period. However, there are occasions when you may wish to sample other groups of cows. When faced with a high incidence of milk fever or retained placenta, it would be best to look at the energy and mineral status of the dry cows and perhaps also a few animals immediately after calving, and analysis for magnesium, phosphorus and selenium might be particularly useful. Copper deficiency is best detected in pregnant heifers, since the requirements of copper for growth and pregnancy are greater than for milk production. Similarly, if you are investigating a possible fatty liver syndrome in your dairy herd, bloods are best taken from cows at seven to fourteen days after calving and analysed for glucose and GOT/AST (aspartate amino transferase, an indicator of liver damage).
A fuller explanation of the metabolic profile test is outside the scope of this book and those interested should discuss it in detail with their veterinary surgeon. The metabolic diseases are described individually in the following section, when the concept of the ‘nutritional imbalance’ should become more apparent.
Milk Fever
This disease is best described by its technical name of parturient hypocalcaemia, which means a lowered blood calcium level around the time of calving. As Figure 6.3 shows, the cow has a massive store of calcium in her skeleton (6000 g) and plenty in the food in her intestine (100 g). She has only a small quantity (10 g) circulating in her blood however. Although this reservoir of readily available calcium is sufficient to meet the requirements of the calf in late pregnancy (8 g/day), it is not adequate to match the huge increase in the requirements of milk production in early lactation (25 g/day). There are always on-going ‘obligatory’ losses of calcium in the urine and faeces (12 g/day), which the cow cannot avoid, and to make matters worse, colostrum contains twice as much calcium as milk (2 g/litre versus l g/litre). There is also a tremendous loss of calcium in the birth fluids.
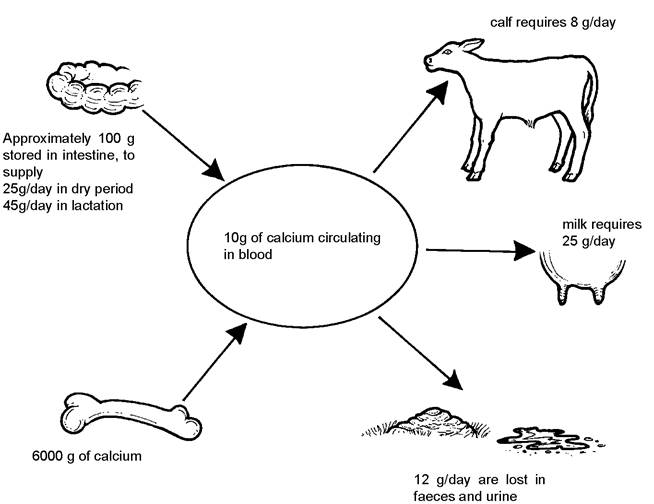
Figure 6.3. Calcium balance within the cow in pregnancy and lactation.
At the point of calving, therefore, there is a very heavy and sudden increase in the demand for calcium and most cows will experience a drop in blood calcium levels. This is compensated for by:
• increased activity of parathyroid hormone, leading to
• increased efficiency of calcium absorption in the intestine, from 35% pre calving to 55% immediately post calving
The effect of this is to increase the amount of intestinal calcium absorbed from 25 g/day to 45 g/day, i.e. a net increase of 20 g. Combined with the 8 g/day no longer taken by the calf, this should be adequate (20 + 8 = 28 g) to compensate for the 25 g/day being drawn into milk production.
Generally only a few cows will be affected by clinical milk fever, so what are the control mechanisms which maintain calcium levels? These are explained in detail in the following.
Mechanisms controlling blood calcium levels
The mechanisms involved are shown in Figure 6.4.
The cow obtains its vitamin D either from the diet or by synthesising it in the skin under the influence of ultra-violet light. Whatever the source, D3 must first go through a primary activation change to 25 hydroxy D3 (25(OH)D3) in the liver. Falling blood calcium levels trigger off a signal which leads to the release of parathyroid hormone. (There are two parathyroid glands on each side of the thyroid gland in the neck, Plate 12.3.) Parathyroid hormone has a limited ability to stimulate calcium and phosphorus release from bone, but its main action is in the kidney where it converts 25 hydroxy vitamin D3 (made in the liver) into the very active form of 1,25 dihydroxy vitamin D3 (1,25(OH)2D3). It is this latter hormone which is responsible for increasing the absorption of calcium from bone and particularly from the gut. The intestine is the major source of calcium around calving: the bone mobilisation mechanisms take some ten to fourteen days to come into operation. This in itself is important, because intestinal muscle is particularly susceptible to low calcium (depressing its activity) and hence milk fever is almost a self-perpetuating syndrome. Low calcium produces a decrease in ruminal movements and hence in food intake and the reduction in intestinal activity further reduces calcium absorption from the gut.All cows show increases in both parathyroid and 1,25 dihydroxy vitamin D3 at calving, and yet some are unable to mount a response which is sufficient to prevent milk fever. The activity of both hormones is
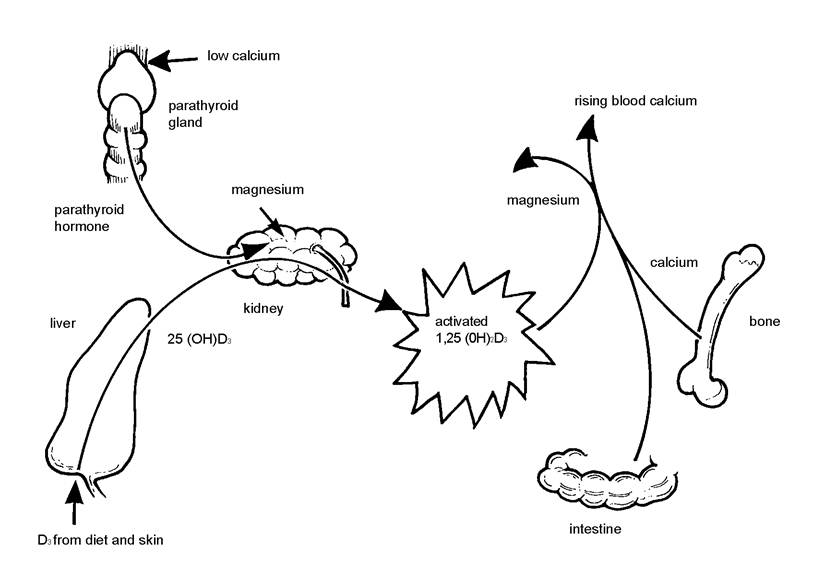
Figure 6.4. Control of blood calcium levels. Parathyroid hormone, produced in response to low calcium, activates vitamin D3 in the kidney and this promotes calcium absorption from bone and gut.
stimulated by the presence of magnesium at the points shown in Figure 6.4 and this is why low magnesium intakes during the dry period can lead to an increase in the incidence of milk fever.
Oestrogens inhibit calcium mobilisation mechanisms and since oestrogen levels rise at calving, this would be another reason why milk fever occurs.An increasing number of high-yielding cows seem to be developing milk fever at six to eight weeks after calving or even in mid lactation. This is usually associated with oestrus (leading to high oestrogen levels) and/or a digestive upset (depressing calcium absorption).
Older cows are much more susceptible to milk fever because they have fewer D3 receptor sites in bone and intestine and hence their calcium reserves are less available. The condition is virtually never seen in heifers and only rarely in second calvers. Cows which have had milk fever at one calving will be more susceptible at subsequent calvings.
Channel Island cattle, particularly Jerseys, are more susceptible than other breeds, and general stress on the cow, in terms of environment, can make the condition worse. Yield is important. Over the ten year period from 1960 to 1970, yields rose by 30% and milk fever incidence increased from 3% to 9%. In underdeveloped countries, where yields are much lower, milk fever is rare.
Clinical signs
In the body, calcium is needed to liberate acetylcholine, a chemical messenger from the nerve ends which activates muscles. Lack of calcium therefore results in a failure of acetylcholine release and the clinical signs of milk fever are essentially those of a lack of muscle function.
In the early stages the cow will be walking stiffly, throwing her legs out to the side in order to retain her balance. She will be slightly blown (lack of ruminal activity) and probably constipated. Later she will be found sitting and unable to rise, or possibly she is only able to half lift herself onto her hind legs and then falls back to the ground again. The list of other possible causes of an inability to stand after calving given in Chapter 5 should be read in conjunction with this section.
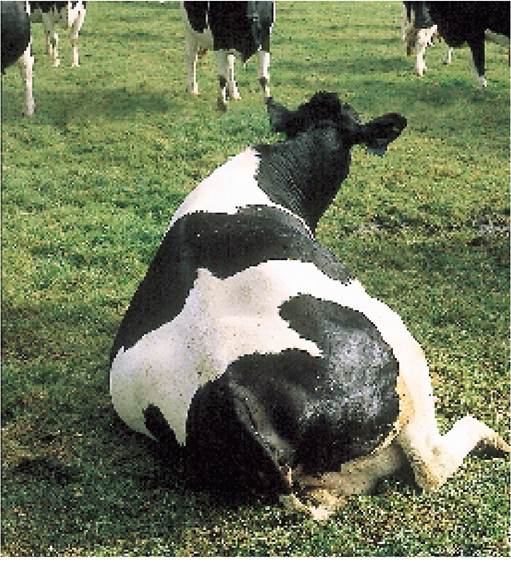
The milk fever cow is quiet and sits with a characteristic ‘S’ shape in her neck (Plate 6.1), rather than holding her head to one side in a slow bend, which is the position you would see in a normal cow (e.g. Plate 5.28). Her coat feels cold, she is likely to be cudding either irregularly or not at all, and this makes her slightly blown. Her temperature will be below normal. The rectum will be full of faeces, making the anus bulge backwards. This occurs because there is insufficient muscle power to enable the cow to defecate, and is a feature clearly seen in Plate 6.1. As blood calcium falls, intestinal movement also decreases and as a result, even less calcium is absorbed from the gut into the blood. Some cows develop a fine muscle tremor, seen as a ‘shivering’ especially over the neck and chest area. If left untreated, the muscle Plate 6.1. Typical position of a milk fever cow. Note the ‘S'neck paralysis worsens and the cow and the rectum bulging with faeces under her tail.
eventually rolls over onto her side and lacks the power to sit up again. When she is on her side the normal rumen
gases cannot escape, so she becomes bloated and death is caused by either excessive pressure on the heart or possibly by inhaling rumen contents which have been forced up into the mouth by the pressure of the gas.
Table 6.1. Cows which have had milk fever are likely to be much slower to get back in calf. There is also an increased risk of acetonaemia.
| Normal calvings | Cows with milk fever | |
| Number of cows | 27 | 30 |
| Percentage cycling by 5 weeks | 32.5 | 12.5 |
| Days from calving to first oestrus | 54 | 71 |
| Days from calving to first service | 67 | 82 |
| Days from calving to conception | 92 | 120 |
| Number of services per conception | 1.7 | 1.9 |
| Incidence of ketosis (%) | 48 | 90 |
| (based on ketones in urine) | ||
| From Bouters 1986. |
These are the general clinical signs of milk fever. What is often not realised, however, is that cows which have had milk fever have a reduced resistance and are therefore much more susceptible to a whole range of subsequent conditions such as retained placenta, mastitis, metritis and fatty
liver syndrome. A proportion will also develop secondary injuries to bones, nerves or muscles and will never get up. Finally, those which do recover will have poorer fertility. Table 6.1 shows that days to first service and the calving to conception intervals are both affected. At a cost of £3.50 per day (1998 values) the extra 28 days from calving to conception, that is the extra time to get a milk fever cow back in calf, will amount to £98 - and this is in addition to the cost of treatment.
Treatment
Calcium is given by injection, usually in the form of calcium borogluconate. Various regimes are used and the important feature is to make sure that the cow receives at least 12 g of calcium in one dose. This may be given as 400 ml of a 40% solution by slow intravenous injection - if given rapidly it can cause a fatal heart failure. The technique is described in Chapter 14. Sometimes blood levels of phosphorus and/or magnesium are also low and if your vet thinks that this is a possibility, then proprietary preparations containing calcium mixed with phosphorus and magnesium should be used. There is less risk of heart failure using the 20% calcium solutions intravenously and they can also be administered subcutaneously, but two 400 ml injections of 20% would be needed. If 40% solutions are given subcutaneously there is a risk of producing a sterile abscess under the skin (Plate 10.29), and this route of administration should therefore be reserved for 20% solutions only. Calcium preparations should be warmed prior to use and subcutaneous injection sites must be massaged afterwards to promote absorption.
As soon as it is practically possible, the cow should be manoeuvred into a sitting position. If she is ‘flat out’, it will be better to try to get her upright while someone else goes to call for veterinary assistance and/or to collect the calcium. Although it is very difficult to do when a cow is blown, try to get her sitting upright, as even a cow with severe milk fever will live for several hours in this position. Bales of straw can be used as supports and it may be necessary to pull her head around with a halter. After the calcium has taken effect, the cow should sit upright reasonably well, although you must make sure that the hind legs are correctly positioned, as shown in Plate 5.28. This is extremely important in order to prevent permanent nerve damage. The first signs that the calcium is working are often a belch, liberating ruminal gas, and defecation, as muscle power returns to the rumen and rectum respectively. It is said that if faeces flow from the blunt end of the cow soon after calcium has been administered to the pointed end, then the diagnosis of milk fever has been confirmed! Encourage the cow to start eating as soon as possible after treatment. This will supply additional dietary calcium and also promote gut activity to facilitate absorption of that calcium. It may even be worth giving a calcium/vitamin D drench (discussed under prevention) to prevent a relapse.
Usually the cow is standing again within a few hours of being given the calcium and the only preventive measure needed then is to make sure that the calf does not suckle too much and that the cow is not ‘milked out’ for one or two days, as this would stimulate increased milk flow and might precipitate another attack of milk fever. In a proportion of cases treatment may improve the general appearance of the cow, but she is still not standing six hours later. This is an instance where your vet shoUld definitely be called. A thorough examination will be given to check that none of the other factors mentioned in Chapter 5 are involved, and blood samples may be taken to see if magnesium or phosphorus levels are seriously low and possibly also to check for liver function and muscle damage. It may be that the cow simply needs a second dose of calcium, and this is often the case, with full recovery occurring one to two hours later. If she remains recumbent, however, she must be moved on to a non-slip surface and nursed as described previously.
Do not give excessive amounts of calcium at any one time. This can produce:
• temporary hypercalcaemia (high blood calcium), thus stimulating production of the hormone calcitonin, which in turn may produce a hypocalcaemia (relapse of milk fever) when the overdose of calcium has been excreted
• death from heart failure. Intravenous calcium will improve circulation in the skin, which can result in rapid absorption of previously administered subcutaneous calcium
Prevention and control
Spring- or autumn-calving herds grazing lush wet pasture may suffer an almost 100% incidence of milk fever. There are four probable reasons for this. Firstly, grass contains a high level of calcium. If the dry cow has been having a high dietary calcium intake, because she only needs a very small amount (8 g per day) for the calf, her calcium mobilisation mechanisms (involving vitamin D and parathyroid hormone) become ‘lazy’. Then when there is a sudden increase in the calcium demand for lactation, she is unable to cope with it. If, on the other hand, instead of grass, she was fed on a low calcium diet during the dry period, her mobilisation mechanisms would be ‘fit and active’, because they have had to work hard to get enough calcium even for pregnancy. In this state she is more able to cope with the sudden demands of calcium for milk production.
Secondly, spring or autumn grass may contain low levels of magnesium and it has been shown that a marginal hypomagnesaemia (that is low blood magnesium levels) can precipitate milk fever. The pasture may also be low in phosphorus, so that although calcium deficiency is the prime problem, low-grade magnesium and phosphorus imbalances are acting as exacerbating factors.
Thirdly, during calving there is a period of gut stasis; that is normal gut movements cease, and this further reduces the cow’s ability to absorb calcium. One of the stimuli for the resumption of normal intestinal activity after calving is the presence of bulky food in the gut and, as all dairy farmers know, lush wet autumn grass passes through the gut fairly rapidly! The incidence of milk fever can be reduced by feeding a quantity of hay, straw or silage to increase the bulk in the intestine, thus improving calcium absorption, both by decreasing the rate of passage of food and by providing a better stimulus for the resumption of gut activity after calving. Not only is intestinal activity depressed at the time of calving, but rumen motility and rumination almost cease. This is explained in more detail on page 170. If rumen movements stop, the cow will stop eating and this further reduces the flow of food (and therefore calcium) along the intestine.
Fourthly, lush grazing produces a high intestinal pH (pH 6.5-6.7) which further depresses absorption of both calcium and magnesium. This is explained in more detail in the section on DCAB that follows.
Some of the more important ways of controlling milk fever, therefore, are as follows:
1. Ensure low calcium intakes during the dry period. Rations as low as 20 g per cow per day have been suggested, but this is virtually impossible, especially if grass is part of the diet. However, it is not uncommon to put late pregnant cows onto a sparse pasture and feed straw plus a special ‘down- calver’ concentrate (low in calcium) as a means of control. Conventional dairy cakes are especially bad in this respect because they contain high levels of calcium. Rolled barley would be a better alternative.
2. Avoid excessive feeding or ‘steaming up’ pre calving, so that the risk of fatty liver is reduced and the
very high early flush of milk production does not occur.
3. Ensure adequate dietary magnesium and phosphorus intakes.
4. Supplement with hay, straw or silage and provide a highly palatable diet to maintain appetite immediately prior to and after parturition, and at this stage supplement with high calcium products.
5. Try the dietary cation-anion balance (DCAB) approach, pioneered by Bede in North America. It is almost the reverse of trying to achieve low pre calving calcium intakes. The system is based on feeding anions to acidify the diet for the three to five weeks prior to calving. This then allows increased calcium absorption from the intestine.
• Anions are negatively charged salts such as sulphur and chloride (which are electrically attracted to the anode).
• Cations are positively charged salts such as sodium and potassium (attracted to the cathode).
The calculation is quite complex, but it involves analysing the ration for these salts (something which is not normally done) and then calculating the dietary cation-anion balance (DCAB) as:
DCAB = (Na+ + K+) - (Cl- + S-) mEq/kg DM
(Na = sodium K = potassium, Cl = chloride S = sulphur, mEq/kgDM = milliequivalents per kilogram dry matter)
The actual equation is
DCAB = (43.5 Na + 25.6 K) - (28.6 Cl + 62.5 S) mEq/kg DM
where the mineral contents are expressed in g/kg DM (see Chamberlain & Wilkinson, page ix).
By having a high (Cl- + S-) relative to (Na+ + K+) the cow develops a mild metabolic acidosis, with acid urine, and this in turn increases the responsiveness of bone and intestine to parathyroid hormone. In other words, calcium mobilisation is increased. Measuring the urinary pH with a dip stick gives an indication of the DCAB: on most diets cows have alkaline urine due to high potassium excretion, whereas this system is trying to achieve acid urine. Because grazing has such high levels of the cation potassium it would be impossible to achieve an adequate DCAB on lush grazing - which is perhaps another reason why we see such high levels of milk fever in cows grazing lush autumn pastures.
Suggested targets for DCAB vary from -20 to -150 mEq/kg DM. This can often only be achieved by careful selection of forages and by supplementing the diet with ammonium chloride, ammonium sulphate and magnesium sulphate. The drawback is that these supplements can make the diet unpalatable (as much as 0.75 kg per cow/day may be needed) with a risk of depressed dry matter intakes.
Caustic wheat (soda grain) and caustic treated straw can have the opposite effect: by increasing the sodium content of the diet, they make the urine very alkaline and the DCAB may rise to +1000 mEq/kg DM. If such diets are fed to dry cows, the incidence of milk fever can increase dramatically.
The DCAB system is said to make it possible to feed high calcium and magnesium diets pre calving (for example, 120 g and 30 g/day respectively) and to feed high concentrates at the same time without any risk of milk fever, fatty liver, displaced abomasum etc. Yields are also said to increase.
Other control measures which can be used are:
6. Give vitamin D3 derivatives by injection. The best of these has the enormous name of 1-alphahy- droxycholecalciferol (1-HCC) and in the UK is marketed under the trade name of Vetalpha. 1-HCC is converted in the liver into the very active form 1,25 (OH)2D3 and hence it avoids the kidney path-
Control of milk fever is based on
• Diet
- ensure low Ca and adequate Mg in the dry period
- increase Ca and Mg immediately before and after calving
- optimise dietary cation-anion balance (DCAB) to acidify the gut and promote Ca absorption
• Management
- avoid flush feeding prepartum
- feed long forage to stimulate rumen and intestine motility
- avoid lush grazing
• Preventive treatments
- give oral or subcutaneous Ca at calving
- inject vitamin D3 or 1,25(OH)2D3 analogues
way which relies on falling blood calcium and parathyroid hormone for activation (see Figure 6.4). Even so, it still takes 18-24 hours for 1-HCC to become activated and its effect starts to wane after 96 hours, although some increase in blood calcium is maintained for up to seven days after injection. Although the product is highly effective, it is still difficult to predict exactly when calving will occur, and this is one of the main problems with this treatment. However, it is widely used. Very high doses of vitamin D3 (10 million units, 30-50 times the normal dose) can also be given, but these take four to five days to work and have to be activated via the liver and kidneys and are therefore less effective. There is also the risk of calcium being laid down in the arteries, a process known as metastatic calcification.
7. Give vitamin D mixed with 100-150 g calcium chloride, either in the feed or as a drench, for four or five days before calving. Calcium is absorbed better from acid gut conditions and this can be produced by adding ammonium and magnesium salts to the ration, or even drenching with 100 ml of 10% hydrochloric acid. Commercial oral preparations containing calcium, magnesium and phosphorus are available, although they are not used routinely, perhaps because of the difficulty in treating cows which are very close to calving as a separate group. They are a useful adjunct to therapy, especially for the recurrent case of milk fever. Adding a bottle of 40% calcium injection to a bucket of warm water and giving it to the cow to drink immediately after calving will also help.
8. If faced with an outbreak, or if certain cows are known to have had milk fever in previous lactations, it is worthwhile giving 400 ml of a 20% calcium solution (preferably with a low level of magnesium and phosphorus) subcutaneously, immediately after calving. This will help the cow over her first four to six critical hours and possibly prevent the occurrence of full-blown milk fever.
9. There is some Dutch evidence that supplementing pasture with sodium helps to control milk fever, because sodium and calcium uptakes from the intestine are linked. This would be contrary to the DCAB principle discussed above.
Hypomagnesaemia (Grass Staggers)
As its name implies, hypomagnesaemia is caused by a deficiency of magnesium in the blood. The disease occurs in beef cows on very bare pastures and in single-suckled calves (Chapter 3), but here we will be confining our attention to the condition seen in milking cows. The balance of magnesium for a dairy cow is shown diagrammatically in Figure 6.5. Although there is some 200 g of magnesium present in the body (much less than calcium), most of this is unavailable and to fill any short-term deficit the cow has an ‘available’ store of only 4-6 g. Consequently she must receive a regular dietary intake to prevent blood levels falling. The absorption of magnesium is not very efficient: only 17% of ingested magnesium is absorbed from the gut, the remainder being excreted in the faeces. The cow also does not have the luxury of increasing her efficacy of absorption in periods of deficit, as she does with calcium.
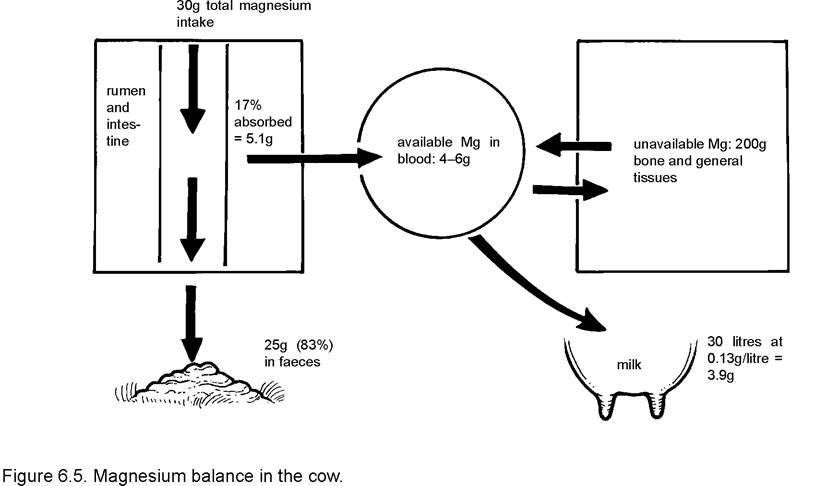
Intake and requirements
Milk contains 0.13 g of magnesium per litre, so a 30 litre cow would have a daily magnesium requirement of 30 x 0.13 = 3.9 g per day (Figure 6.5). Lush grazing could contain as little as 0.1% magnesium in the dry matter, so a cow eating 18 kg DM daily would be receiving only 18 g of magnesium, of which only 17% (3.1 g) is available - not enough to satisfy her requirements. Hypomagnesaemia could develop within a few days. However, this is a very low pasture magnesium value.
The level of magnesium obtained from the forage is depressed by factors such as:
• heavy nitrogen fertiliser
• modern rapidly growing swards. The inclusion of clover helps in correction
• high potassium in the soil: the use of potassium fertilisers should be avoided
• lush low fibre and high nitrogen result in a rapid passage through the gut and an increased ruminal pH, both of which further decrease magnesium absorption (most of the magnesium is absorbed in the rumen)
• low dietary sodium. The absorption of magnesium (and calcium) from the intestine is partly dependent on sodium, and if herbage sodium goes below 0.3% (see Table 12.1), the rate of magnesium absorption will fall
Clinical signs
One of the functions of magnesium in the body is to act as an electrical suppressant of nerve and muscle activity. The symptoms of deficiency are therefore the reverse of this, that is excitability. In the early stages the cow will have an erratic, slightly stiff-legged walk, with her head held high and her eyes wide and staring. If she is suddenly excited, or even if she is driven for any distance, she may fall over and go into hypomagnesaemic tetany: her legs will either be stiff and in spasm, or they will be paddling violently. Her head will be straight, her eyelids ‘fluttering’ if you approach them with your hand and she is likely to be frothing at the lips and ‘chomping’ with her mouth. The ‘wild’ eye and frothing are two features clearly recognisable in Plate 6.2. A proportion of cows are simply found dead, the excitement hav-

Plate 6.2. Hypomagnesaemia. Note the wild frightened look in her eye and frothing at the mouth.
ing produced heart failure, but even then the presence of extensive struggling and paddling marks on the ground where she has been found lying may give a clue as to the cause of death.
Treatment
If hypomagnesaemia is suspected, try to avoid exciting the cow and precipitating a session of tetanic spasms. Magnesium therapy, usually as 400 ml of a 25 per cent solution of magnesium sulphate, should be given immediately. If you have some to hand, administer a bottle subcutaneously - if given intravenously it will precipitate a fatal heart attack. At the same time, and especially if the cow is showing spasms, veterinary assistance should be sought. Your vet will be able to administer sedatives such as barbiturates to calm the cow, thus reducing the risk of a heart attack, and will probably give a mixture of magnesium and calcium by slow intravenous injection, monitoring the heart as he does so. He will also want to discuss the relevant control measures for the remainder of the herd.
Following the administration of magnesium and sedatives, the excitability of the cow is soon reduced. She should then be propped upright, putting her legs in the correct sitting position to avoid muscle damage, and drenched with 60-90 g of calcined magnesite, or some similar preparation, to restore intestinal magnesium levels.
Prevention and control
Magnesium is not stored in the body and control is based on providing a regular daily intake during the period of risk, that is whenever the cows are grazing lush young pasture. In the UK this occurs especially during May and early June, and can also be a problem in September. Outbreaks of disease are seen particularly following stress, for example on a very cold, wet day, when the cow’s energy intake is also reduced. Hypomagnesaemia is also more likely to occur in cows which are mobilising large amounts of body fat and hence there may be an association with fatty liver syndrome. There are numerous methods of improving magnesium supplementation and you will need to choose the system best suited to your own farm routine:
1. Increase the calcined magnesite level in the concentrate to 60 g in 5.5 kg. Unfortunately this reduces its palatability and may lead to refusal by some cows. Others, particularly those on a higher level of feeding, may scour. However, the main problem is that when ample grazing is available, it is uneconomic to feed high levels of concentrate.
2. Magnesium supplementation of the drinking water. This is probably the best method of control since the higher-yielding cows who need more magnesium will be drinking more water and will hence receive a higher intake of supplement. Usually a concentrated solution of magnesium acetate is used and this can be added to the water trough by hand, or by means of proportioners. The latter may be fitted to the mains supply, thus medicating the drinking water for the whole farm, or there are simple and relatively inexpensive devices which can be attached to individual water troughs. One such device is shown in Figure 6.6.
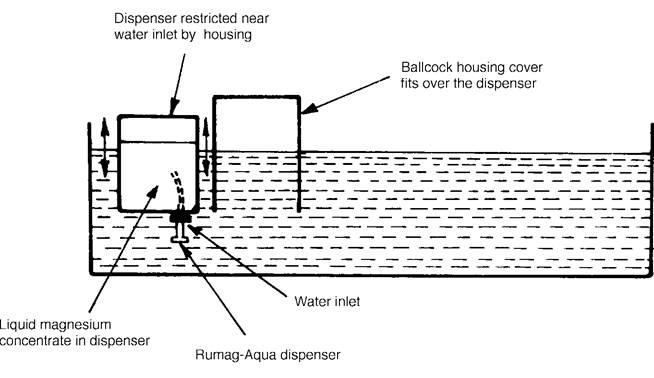
Note: Water flow rate into the trough must be adequate. If the dispenser falls onto its side, it ceases to dispense.
Figure 6.6. The Rumag-Aqua dispenser, a method of adding magnesium to the drinking water.
A much cheaper, but somewhat less accurate, method is to use commercial magnesium chloride, which is approximately 50% pure. A reasonable dose would be 60 g per cow per day, but this of course depends enormously on how much magnesium is being obtained from grazing and other foodstuffs. To obtain the full 30 g per day requirement, a 30 litre cow would need to consume 120 g per day of magnesium chloride. Put the daily amount required by the herd into a fertiliser sack, add some stones and then tie the top. Punch 8-10 holes in the sack, and then place it in the water trough. The magnesium then diffuses into the water. It should be stressed that this is not an accurate method, but by supplementing the drinking water it does mean that all cows receive an additional intake.
3. Hypomagnesaemia can also be controlled by feeding dry forage (hay or straw) each day before turnout onto the lush grazing of spring or autumn. This is a good practice generally, since it helps to reduce the risk of bloat and milk fever and offsets the reduction in butterfat which often occurs, as well as controlling hypomagnesaemia by reducing the rate of passage of food and preventing high ruminal pH levels. Buffer feeding (also known as storage feeding), whereby cows are fed silage throughout the spring and summer grazing, is an even better preventive measure.
4. Improve the magnesium content of the sward. This can be done in four main ways, namely:
• Use a clover mixture, since clover has a much higher magnesium content than grass.
• Add calcined magnesite to the soil at the rate of 250 kg per acre. This has an effect only on sandy or low pH soils.
• Avoid using high potassium fertiliser on pastures which the cows are going to graze in spring and also avoid grazing pastures which have had heavy applications of slurry during the winter (both slurry and straw-based manure have high potassium levels). A high potassium content in the soil significantly reduces magnesium uptake by the plants and hence increases the risk of hypomag- nesaemia.
• Regular liming maintains the correct soil pH and improves magnesium uptake. A general discussion on methods of increasing soil and pasture mineral levels, and on supplementation in general, is given in Chapter 12.
5. Pasture dusting: spreading calcined magnesite over the pasture every second or third day, using an artificial fertiliser distributor, works quite well, although it is fairly laborious and entails driving over the grazing. It should be applied at a rate which will provide an intake of 60 g per cow per day.
6. Free-access high-magnesium minerals will undoubtedly help, but some cows will take far more than they need (probably because they like the taste of the salt added to it), while others will take nothing and be at risk. This is a good example of the fallacy of the statement that ‘cows take whichever mineral they need’ (for a fuller discussion of this method of mineral supplementation, see Chapter 12).
7. Magnesium bullets: these are large, cylindrical, metallic objects which, given by mouth, lodge in the bottom of the reticulum where they slowly dissolve, releasing magnesium at a controlled rate each day. Their weight keeps them in place, although in a small proportion of cows they are regurgitated with the cud and these animals are then at risk. Generally two bullets are given to reduce this risk and they supply magnesium to cover a two month period.
Because of the risk of rapid death from hypomagnesaemia, some form of additional magnesium supplementation should always be given when the cows are grazing lush spring pasture. However, one of the problems is defining the period of risk and this can only be done by sampling those cows which are most susceptible, that is, the highest-yielding cows receiving no concentrate. Your vet can take blood samples to check magnesium levels, although analysis of urine is even better. Not only does urine analysis give advance warning of impending hypomagnesaemia, but it also indicates when magnesium supplementation is excessive, in other words, when it can be reduced or discontinued. In this way expense may be saved without putting the cows at risk.
Winter hypomagnesaemia
Chronic low-grade hypomagnesaemia has become increasingly common in grass silage-fed dairy herds over the past few years. Although associated production problems have not always been identified, some herds seem to improve in food intake and milk yield when magnesium supplementation is given. Winter hypomagnesaemia is often detected on the metabolic profile test.
Acetonaemia (Ketosis)
Acetonaemia, which is also called ketosis or slow fever, occurs in higher-yielding cows in early lactation. To appreciate why the disease occurs and also what causes fatty liver syndrome, we need to understand a little of the biochemistry of the metabolism of the cow. This is given in outline in Figure 6.7.
High-carbohydrate starch type foods, e.g. barley or wheat, are broken down by the ruminal micro-organisms into a simple acid, propionate, and this is carried to the liver, where it is used to produce glucose. The main function of glucose is in the synthesis of milk and in fact the rate of milk production is largely determined by the rate of supply of glucose to the udder. This is why glucose is one of the metabolites measured as an indicator of energy status in the metabolic profile test. Propionate has a second
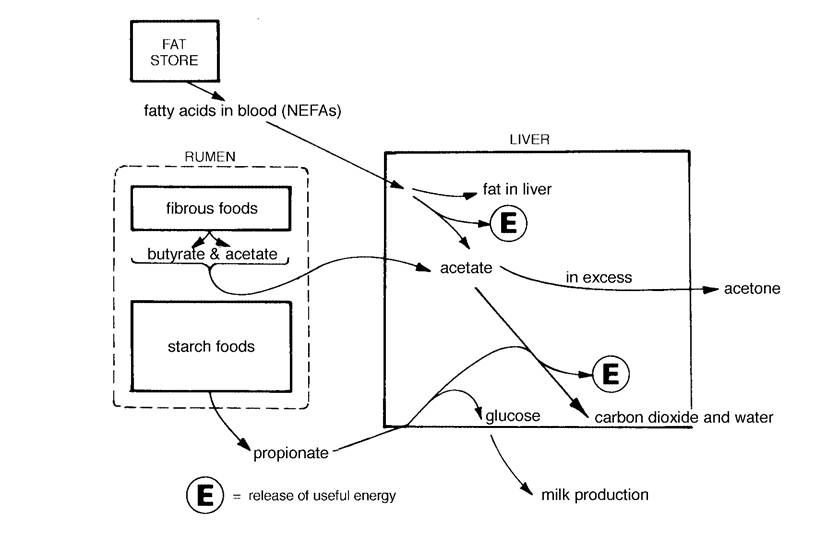
Figure 6.7. Energy metabolism in the cow.
function, however, and that is its involvement in fat metabolism, or more precisely in the release of useful energy (E in Figure 6.7) from fat. The cow in early lactation is unlikely to be able to consume sufficient energy in her diet to meet the needs of milk production and so she sends out an alarm signal to her fat stores. Fat is broken into small blocks, the fatty acids. They can also be measured in the metabolic profile test when they are known as NEFAs, i.e. non-esterified fatty acids, and these are carried via the blood to the liver. Once in the liver they are broken down to acetate (or acetic acid) and this releases considerable quantities of useful energy E. However, the complete degradation of acetate to carbon dioxide and water with the release of further energy requires the interaction of propionate. The diagram also shows that fibrous foods (hay, etc.) are decomposed by the ruminal micro-organisms into acetate and butyrate. These two metabolites pass directly to the liver; the butyrate is converted into acetate, further increasing the cow’s requirements for propionate.
If the cow is not being adequately fed, her total propionate production will be converted into glucose and used for milk production. There is still a signal going out for the mobilisation of fat to produce energy, however, but because there is no further propionate available, fat metabolism cannot proceed beyond the acetate stage, and the excess acetate accumulates in the liver. After a while the liver is unable to store any further acetate, and to dispose of it two molecules of acetate are combined to produce acetone. The acetone passes from the liver into the blood, where it acts as an intoxicant to the cow, producing the symptoms of acetonaemia. The word literally means acetone in the blood, and it is effectively caused by an inadequate intake of starchy food in a cow which is already mobilising body fat. Other ketone compounds formed from the excess acetate include acetoacetate and beta-hydroxybutyrate. The latter compound is also used as an indicator of energy status in the metabolic profile test. High blood levels of beta-hydroxybutyrate indicate a dietary energy deficit.
Clinical signs
Acetonaemia is seen primarily in higher-yielding cows and the first symptom is likely to be a partial or total refusal to eat concentrate, although the cow will probably continue to eat some hay or silage. She then becomes very dull and lethargic, and hence the name slow fever. After a short while, rumination virtually ceases, the dung becomes dry and hard, and milk production falls. In a proportion of cows the acetone can affect the brain and these animals become excitable, froth at the mouth, lick objects excessively or stand with their heads raised and pushed into a corner. The Guernsey cow shown in Plate 6.3 had several relapses of acet- onaemia. She was unsteady on her legs and tended to go round in circles, drooling from the mouth and biting at her shoulder. Excessive biting and licking (Plate 6.4) are commonly seen with the nervous form of ketosis. Some cows may even collapse in the parlour, resembling hypomagnesaemia. However, the most common clinical signs are a drop in yield, poor appetite, dullness and constipation, which is the result of excessive fluid loss from the body producing very dry dung.
The best diagnostic sign is the smell of acetone on the breath, which has a ‘sharp’ scent, like pear-drops. If you are in doubt, try sniffing the breath of a normal cow, then the breath of an affected cow and finally a bottle of nail varnish remover, which is neat acetone!
Treatment
Because there are other conditions, for example, displacement of the abomasum (see Chapter 13) which can lead to secondary acetonaemia, you would be well advised to seek veterinary advice for the diagnosis and treatment. The treatment prescribed will most probably consist of three components. Firstly drugs given by injection, to stimulate an increase

Plate 6.3. Nervous ketosis (acetonaemia). This Guernsey cow walked round in circles, drooling from the mouth and biting her shoulder.

Plate 6.4. Nervous ketosis. This cow was biting herself and would try to eat her owner's hand! Note her sore nose, due to excessive licking, and her glazed eyes. She was almost blind!
in blood glucose levels and to boost the rate of liver metabolism generally. These drugs will be of the
steroid or glucocorticoid groups.
Secondly, substances can be given by mouth to boost blood sugar levels and to improve metabolism. Probably the most common are sodium propionate, propylene glycol, and glycerol, which are chemically closely related. Reference to Figure 6.7 shows how propionate can combine with the excess acetate in the liver, allowing its full metabolism to carbon dioxide, water and energy. This will not only reduce blood levels of acetone, but it will also allow the release of considerable quantities of energy from the acetate, and in so doing it overcomes the primary defect of acetonaemia. Glucose will only be beneficial if given by intravenous injection. If given by mouth it is decomposed by the ruminal micro-organisms.
Finally, altering the ration of sick animals and feeding them individually will help. Sometimes affected cows will eat barley, sugarbeet pulp or fodder beet, but not proprietary dairy cake, with its higher protein content. Molasses may also be palatable.
Prevention
As acetonaemia is caused by an energy intake which is inadequate to meet the demands of milk production, then clearly prevention and control of the disease are based on maintaining a correct diet. The ration must contain sufficient readily available energy to meet the needs of metabolism as described in Figure 6.7; that is, a reasonable intake of cereal products or proprietary concentrate. If the forage is of poor quality (poor hay or silage), then additional concentrate needs to be fed to balance this and, as a rough guide, the M/D of the overall ration for a high-yielding early lactation cow should not fall below 11.0 MJ/kgDM. Especially dangerous are rations containing excessive fibre levels, silage with poor palatability, e.g. with a butyric fermentation, high nitrogen levels, or diets with a gross excess of protein. These factors can lead to outbreaks of aceton- aemia, with quite large numbers of cows affected. If apparently normal cows from such herds were blood sampled, e.g. as part of a metabolic profile, they would have low glucose levels, high acetones and high levels of non-esterified fatty acids (NEFAs) and beta-hydroxybutyrate in their blood.
Acetonaemia can also occur in individual animals and here it may be management which is at fault. Possible causes include inadequate feeding space, so that the smaller cows or heifers get pushed away and do not receive their fair share. Secondly uneven distribution of the daily feeds can lead to some cows being unable to cope, while those with larger appetites can compensate. A third cause is cows which are overfat at calving because excessive fatness leads to reduced appetites in early lactation, thus making them more susceptible to acetonaemia. This may occur as an individual or a herd problem.
Sometimes there is a primary failure of the liver, so that the cow is unable to carry out her metabolic functions correctly. Chronic liver fluke would be a good example, or the fatty liver syndrome which is discussed in the next section. The conversion of propionate to glucose and the complete oxidation of acetate to carbon dioxide and water both occur in the liver cells, and hence liver damage can predispose to acetonaemia.
Acetonaemia (ketosis) may be caused by
• low starch/energy in the ration
• unpalatable feeds
• inadequate feeding space
• overfat cow at calving
• secondary to displaced abomasum, etc.
Fatty Liver Syndrome
The cause of this clinical disorder is very similar to that of acetonaemia. Research has shown that even normal cows can have quite a high proportion of fat stored in their liver cells immediately prior to calving. Then, with the stimulus of milk production, a signal is sent out calling for mobilisation of fat from the fat stores of the body to meet the energy deficit. This was explained in Figure 6.7. When the fat arrives in the liver, there may already be a backlog of acetate and so surplus fat is stored in the liver cells until it can be used. Eventually the amount of fat stored reaches such a high level (up to 60% of the space inside the liver cell) that the liver’s normal functions, including acetate metabolism and the conversion of propionate to glucose, are seriously retarded. This means that the rate of acetate utilisation is further reduced and even more fat accumulates. All aspects of liver function are now affected and in the extreme case the cow simply degenerates into a condition of acute liver failure. A lesser degree of fatty liver seems to be common in many dairy herds. One survey showed that in 40% of the cows sampled at one to two weeks post calving, more than one-fifth of the space within their liver cells was occupied by fat.
Clinical signs
The severe disease of total liver failure is often precipitated by some other condition, quite commonly an unresponsive case of milk fever. While the cow is on the ground her appetite will be reduced and so she
| has to mobilise fat from her reserves to her liver to meet her energy requirements. Some animals continue to eat and drink and generally look | Table 6.2. The effects of fatty liver on fertility and disease incidence. | ||
| Normal | Fatty liver | ||
| bright. Others become dull and depressed and, after a day or two, stop eating - these may be the liver failure cases. Their eyes become dull and | 1. Calving to: | cows (less than 20% fat) | cows (greater than 20% fat) |
| they cease to notice your approach or | first ovarian activity | 20 days | 30 days |
| any other movements around them. | first observed oestrus | 50 days | 70 days |
| They tend to sit with their heads twisted around to one side, almost touching their hind feet, and they may then start to make small moaning and | services per conception 2. Incidence of disease in 17 experimental cows: | 1.6 | 2.4 |
| groaning sounds with each laboured | ketosis | 2 | 5 |
| breath. Any movements are uncoordi- | mastitis | 1 | 6 |
| nated and severely affected animals | retained placenta | 1 | 1 |
| roll over onto their sides and are | cystic ovaries | 0 | 2 |
| unable to sit up, even with assistance. At this stage the prognosis is hopeless | milk fever | 1 | 2 |
| and no treatment will be of any value. Blood samples taken in the early stages would give very high GOT/AST values, indicating liver | Total disease incidence | 5 (in 9 normal cows) | 16 (in 8 fatty liver cows) |
| damage. Such severe manifestations of fatty | From Reid I. & Roberts J. (1982), In Practice 4 164. | ||
liver are only the tip of the iceberg.
Many cows are now known to be mildly affected, so that various important liver functions are depressed, simply because of the bulk of fat present in the liver cell. Probably the most significant of these is the effect on subsequent fertility. The protein albumin is manufactured in the liver. Its rate of production is depressed in cows with fatty liver syndrome and blood albumin levels fall. Research has shown that cows with low blood albumin levels after calving will have a reduced conception rate when they are served later in their lactation. Table 6.2 shows a survey which grouped cows into those with ‘normal’ levels (20% fat). The difference in the subsequent fertility of the two groups is quite startling. Cows with fatty livers are also more susceptible to infectious disease and to other metabolic disorders. This is clearly demonstrated in the second part of Table 6.2 which shows the incidence of disease in an experiment in which eight cows developed fatty liver and nine cows remained normal.
Prevention
Cows should be fit but not fat in late pregnancy and must be fed well in early lactation to avoid excessive weight loss. Diet is therefore extremely important in control and these points have already been mentioned in relation to acetonaemia. Not only do overfat cows (body score 4.0 and above) have excessive fat in their liver cells, but they will also have reduced appetites in early lactation, thus exacerbating their energy deficit. Cows calving in condition score 2.5 to 3.0 are probably ideal. Providing a small quantity of the post calving ration for the final one to two weeks pre calving will help. This will acclimatise the rumen microflora to the new diet, and it also helps to compensate for the reduction in feed intake seen in most cows during the few days prior to calving. Those who use the DCAB system (page 160) consider that quite high levels of feed can be given pre calving. Avoid gross overfeeding of concentrates in very early lactation. This can lead to acidosis, with a consequent ruminal atony and depressed food intake.

Acidosis
Acidosis could be considered as a metabolic disorder, although some would say that it is simply a digestive upset. Cattle fed all-forage rations have a pH in their rumen of around 6.0-6.5, and the products of microorganism fermentation are acetate (70%), propionate (20%) and butyrate (8%) in approximately the proportions shown. Following a feed of concentrate, that is highly fermentable carbohydrate, certain types of bacteria proliferate to produce lactic acid and this results in a fall in rumen pH. If the acidity reaches pH 5.5, there is likely to be a reduction in rumen motility, in other words the rumen stops contracting (Appendix One). This results in a loss of appetite, especially for forage, and she may not eat anything for one to two hours after a large feed of concentrate.
Greater reductions in ruminal pH, for example to pH 5.0, can result in quite severe signs of ill health. The acid rumen inhibits cellulolytic (cellulose digesting) bacteria, and many of the protozoa are killed. This means that only starch fermentation continues, thus making the syndrome worse. When the pH reaches 4.5-4.0 death is likely. The lactic acid concentration in the rumen is so high that the
Plate 6.5. Rumen acidosis, in this instance caused by overeating fodder beet. Note the red, inflamed rumen wall and the way in which the black rumen lining is peeling off.
| The importance of rumen pH | Effect | |
| pH | ||
| normal mild acid | 6.0-6.5 5.5-6.0 | good rumen function reduced rumen motility and forage intake; poor cellulose digestion |
| moderate acid | 5.0-6.0 | sick cow; scouring |
| severe acid | 4.0-4.5 | death likely |
rumen wall becomes inflamed and the lining starts to fall off (Plate 6.5). Fluid is drawn in from the circulation by osmosis, blood pressure falls and shock sets in. This is classically referred to as the overeating or starch overload syndrome and is described in detail (as is rumen function) in Chapter 13.
Some of the lactic acid will be absorbed from the rumen and pass into the bloodstream. This produces metabolic acidosis. In this example metabolic acidosis is therefore secondary to rumen acidosis. Metabolic acidosis can also be secondary to other syndromes, for example calf scour (Chapter 2). Cows are particularly susceptible to acidosis around parturition. Figure 6.8 shows that all cows have depressed rumen movements at the time of calving. We know this: if you do your late evening check on the calving yard and all the cows are sitting chewing their cud, then you know you can go to bed without worrying!
After calving the rate at which rumination starts to return to normal is considerably affected by diet. Diets high in long fibre promote good rumination. High concentrate diets do not. The cow normally overcomes excess acidity in her rumen through the buffering effects of the bicarbonate and phosphate in her saliva. Saliva is produced when the cow chews the cud, i.e. when she ruminates. Failure to chew the cud will lead to reduced saliva production and the rumen becomes more acid. Increased rumen acidity depresses rumen motility, which in turn depresses food intake and especially intake of the long fibre which is so essential for stimulating rumen movements. The whole process of rumen motility and rumen acidosis is intimately connected to the natural depression of rumen movements around the time of calving, and as such it is essential that adequate long fibre is included in the ration, particularly at the time of calving. This is sometimes referred to as the scratch or tickle factor of the diet. A healthy functioning rumen means a healthy cow.
Straw is probably the best feed to achieve this and it is interesting that many dairy farmers are now feeding increased amounts of straw to dry cows, and are also incorporating 1-2 kg of long chopped straw in the production ration. Rumen acidosis has an effect on lameness, particularly sole ulcers and white line abscess (see Chapter 9). The highest incidence of lameness occurs eight to twelve weeks after calving and this is thought to be associated with the stress of calving.
Probably the worst scenario is seen on those farms where cows are put onto full concentrate immediately after calving, when rumen motility is already in a depressed state. At this stage high concentrate intakes can:
• further depress rumen motility
• this then depresses food, and particularly forage, intake
• if the cow continues to milk, her early lactation energy deficit will be severe. The risk of fatty liver and other post-partum diseases (see Table 6.2) then increases enormously
Clinical signs
How would you recognise the presence of acidosis in your cows? The main symptoms are:
• an increased incidence of digestive upsets, for example cows intermittently off-colour and down in milk for a few days
• loose faeces, often with a slightly yellow appearance, and in more extreme cases having a characteristic sickly, foetid smell. Ideally a cow pat should form a discrete, solid mass, with a ‘poached egg’ upper surface, as in Figure 6.9. Very loose dung which spreads across the floor can be a sign of acidosis, although, of course, it can be associated with a whole range of other factors increased respiratory rate, with a sweaty matted coat, rather than the sleek smooth appearance we would expect to see in an early lactation cow
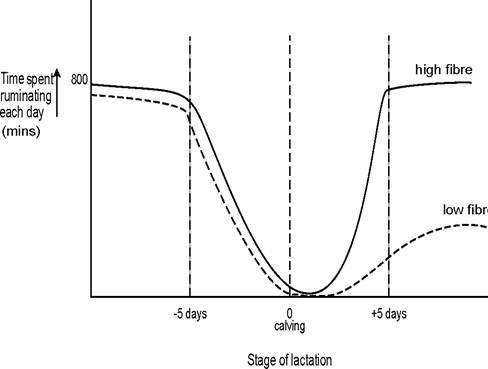
Figure 6.8. All cows show a reduction in time spent ruminating around calving. Increased long fibre diets encourage a more rapid return to normal rumination.
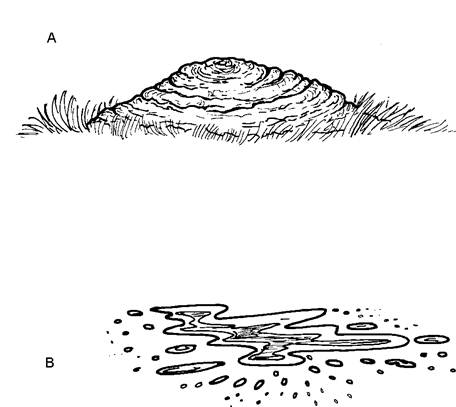
Figure 6.9. A normal dung pat (A) should be well formed, looking almost like a poached egg. Very loose faeces (B), which spread across the floor, can be a sign of acidosis.
regurgitation of the cud. Dropped cuds (irregular masses of partially chewed fibrous food), approximately the size of a small fist, may be found in the collecting yard or at the front of the cubicles. A typical example is seen in Plate 6.6. The addition of 1-2 kg of straw or hay to the ration, or access to big bale silage, invariably stops this within a day or two increased tail-swishing. Some say that acidosis produces acid urine, which in turn leads to an inflamed vagina. The constant tail-swishing can lead to soiling on the back of the cow, as seen in Plate 6.7 severe acidosis can produce acute laminitis, seen as a cow tender on all four feet. The hooves will be hot and a strong pulse can be palpated in the leg. This will produce an increase in foot problems (sole ulcers and white line abscess) one to two months later
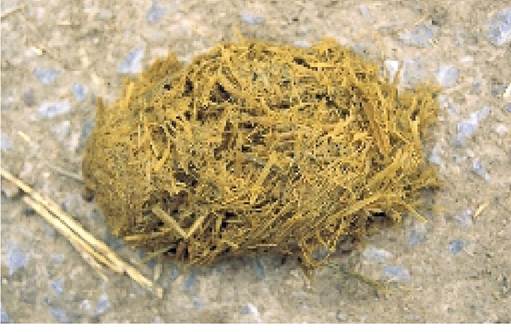
Plate 6.6. Cud regurgitation can be a sign of acidosis.
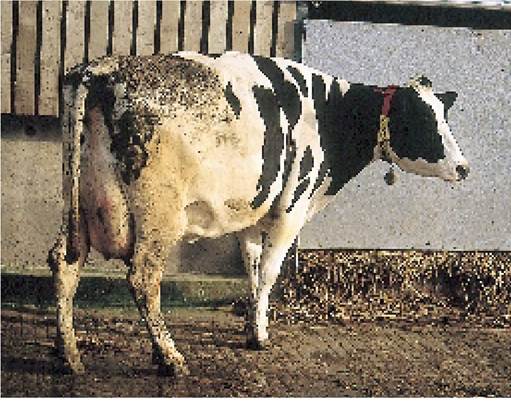
Plate 6.7. A dirty back, as seen in this recently calved cow, can be a sign of acidosis. The dirty back can be due to tail-swishing arising from a vagina irritated by acid urine.
ecules end to end in a long chain (see page 173). If the acid rumen is due to excess concentrate and
starch overload, then there will be high levels of propionate in the rumen, but low acetate, and this
leads to low milk fat
depressed milk fat levels. Butterfat is formed by joining acetate mol- depressed fibre digestion. The protozoa (rumen micro-organisms) which are responsible for digesting cellulose are unable to function in an acid environment. In fact in severe acidosis they are killed off altogether, which is why it may take several days for cows affected by ‘overeating’ to regain their appetite
Prevention
The main way of preventing acidosis is to ensure that the ration contains a reasonable balance between starch and digestible fibre and that there is sufficient long fibre/roughage being eaten to stimulate good rumen activity and hence saliva and sodium bicarbonate production. In more detail this can be achieved by:
• maintaining a minimum of 40% forage in the ration. It is ideal to add 1-2 kg of long-chopped straw to a complete mix. If the straw is chopped too short, it will not provide sufficient stimulation for rumen motility. If it is too long, cows may well leave it at the bottom of the trough. Although straw can be offered on free access, this is by no means as good as mixing it in with a complete ration so that the cow eats the straw with the concentrates, which is ideal
• ensuring an adequate balance between starch (e.g. barley and wheat) and digestible fibre (e.g. sugarbeet pulp or cotton seed) in the diet. Although both starch and digestible fibre are sources of energy, the starch ferments much more rapidly in the rumen, promotes propionate production and increases milk protein. Digestible fibre gives a slower and more sustained release. Both are necessary for good digestion. Note the difference between physical fibre to promote rumen motility and digestible fibre to slow the rate of fermentation in the rumen. It is often said that more attention should be paid to feeding the rumen and less towards feeding the cow. Achieving the correct balance of fibre levels is one way to do this. Medium to high energy foods are available in which the energy source comes mainly from digestible fibre. Examples include sugarbeet pulp, citrus pulp and maize gluten (only about 50% of its energy is digestible fibre)
• spacing the concentrate feeds as evenly as possible throughout the day. This is best achieved in a total mixed ration (complete diet). Feeding systems where high levels of concentrates are fed in the parlour twice daily only are dangerous. There may well be a period of one to two hours of rumen inactivity after each feed. Parlour concentrate intakes in excess of 4.5 kg per feed should be avoided
The type of concentrate chosen and its starch level should depend on the quality of the basic forage. If the forage is already high in fermentable sugars and starch, then a concentrate high in digestible fibre will be needed. If it is a lower quality silage, then a higher starch concentrate will be needed as a ‘food source’ for those rumen micro-organisms which have to digest the forage.
Factors Affecting Milk Quality
The quality of milk is not strictly a metabolic disorder, but I have included it in this section because it is strongly influenced by diet and feeding practices. The average composition of typical Holstein- Friesian milk is given in Table 2.1. The main components are:
water 87.5%
butterfat (BF) 3.8%
solids not fat (SNF) 8.6% = 3.2% protein (2.6% casein, 0.6% albumin + globulin)
4.7% sugar (lactose)
0.7% ash (minerals, including calcium)
To a certain extent the levels of fat and protein for a lactation are established during the first six to ten weeks after calving. If milk quality is poor at this stage, then it is quite difficult to achieve an improvement later in the lactation and it may not be until the following year that full correction occurs. Total yield is similarly affected.
Diet is probably the major factor affecting milk quality. Fibrous foods (e.g. hay and silage) are degraded by the ruminal micro-organisms to produce acetate, and butterfat consists of long chains of acetate molecules joined end to end. On the other hand, the rate of production of milk protein, which is also synthesised in the udder, is dependent on the availability of glucose, and therefore on the level of propionate production from starchy foods in the rumen (see Figure 6.7).
Inadequate long fibre or excess concentrate in the ration leads to low butterfat levels. If silage is young and of a very high digestibility, the provision of 1-2 kg of hay or straw is beneficial. This applies especially when turning out to lush grazing in the spring or autumn. A minimum of 2 kg of long fibre is required for the average cow.
Conversely, diets with inadequate energy or excess fibre lead to low milk protein. This is common in herds fed hay or poor-quality silage, unless the ration is supplemented with sugarbeet, potatoes, barley or some other energy source, although fodder beet seems particularly beneficial. Surprisingly it is the protein fraction of the milk protein which is reduced with low energy rations. Inadequate dietary protein, especially insufficient undegradable protein, can reduce milk protein, but has less effect than the energy content of the ration. Ruminal acidosis can also affect milk quality as described in the previous section.
Protected fats, that is fats which have been treated to prevent them being broken down by the ruminal bacteria, can be added to the ration up to about 1 kg per cow per day, or about 7% in the concentrate. They pass directly into the small intestine, where they are absorbed and then used by the udder to produce butterfat. They will produce a rise in butterfat, but if too much protected fat is included, milk fat and protein levels will fall. By coating both the rumen micro-organisms and the particles of food with a thin layer of oil, high dietary fat levels have an overall inhibitory effect on rumen function. The fat content of the total diet should not rise above 4.5%. This is particularly the case if unsaturated fats (oils) are being used.
Part of the effect of nutrition on milk quality is determined during the dry period. Cows which calve down in poor condition may suffer a depression of around 0.1% protein and 0.2% butterfat and this can persist throughout the lactation. You should aim to calve the cows fit but not fat, that is at a body score of 2.5 to 3.0. Higher than this can lead to fatty liver.
Before leaving the effects of diet on milk quality, it ought to be pointed out that some of the factors which lead to high yields will automatically lead to a reduction in quality. Part of this is simply due to the dilution of milk, although payment systems over the past few years in the UK have placed increasing importance on quality, partly because a greater proportion of milk is being used for manufacture rather than liquid sales.
The main diseases affecting milk quality are parasitism and mastitis. Fluke, worms and even a very heavy louse infestation will all reduce butterfat and milk protein, although the most common is the effect of fluke on milk protein. Mastitis leads to a decrease in lactose and a reduction in milk casein, although overall milk protein may remain constant because the reduction in casein is counteracted by increased globulins. For example, a herd with a cell count of 750,000 cells/ml is probably losing 0.5% lactose, 0.4% casein, 0.3% butterfat and yields will be depressed by 750-900 litres per annum (see Table 7.2). The control of cell count is covered in Chapter 7.
Both butterfat and, to a much lesser extent, milk protein are inherited characteristics, so breeding can have a significant long-term effect. Bulls should be chosen with a high milk-quality performance and poor cows should not be used for breeding. As the genetic variation in butterfat is much greater than for protein, breeding for improved protein status is likely to produce a slower response than breeding for butterfat. Milk quality is generally highest in heifers, falling with increasing age to about the fifth lactation, when it remains approximately constant. It is also lowest at peak yield (probably a dilution effect), although the improvement in quality in later lactation is greater in pregnant than in non-pregnant animals. A large number of cows reaching peak yield in November, combined with the final batch of late calvers being dried off, is a common cause of a reduction in milk quality in autumn-calving herds. Aiming for a well-fed, young herd, paying attention to mastitis and parasite prevention and keeping a tight control on breeding and fertility should all help to maintain a satisfactory milk quality status.
More on the topic A metabolic disease, or metabolic disorder, is the name given to a group of illnesses in dairy cows which are caused by an over-exertion of their normal metabolism.:
- Metabolic Conditions Usually Affecting Calcium or Phosphorus Metabolism
- METABOLIC DISORDERS IN NEWBORN
- Ecological Marx and the Metabolic Rift
- METABOLIC MYOPATHIES
- Metabolic Neuropathies
- Antiretroviral Therapy and Metabolic Disorders
- Metabolic Disorders
- Definition of the Metabolic Syndrome in Non-HIV-Infected Patients
- NUTRITIONAL, METABOLIC AND TOXIC DISORDERS
- Metabolic Liver Diseases
- Chapter 6 METABOLIC DISORDERS
- GENETIC, METABOLIC, AND OTHER DISORDERS
- NUTRITIONAL AND METABOLIC DISORDERS
- NUTRITIONAL, METABOLIC, AND TOXIC DISORDERS
- Pathogenesis of Antiretroviral Treatment- Associated Metabolic Syndrome
- Description and Pathophysiology of the ART-Related Metabolic Alterations
- Prevalence of the Metabolic Syndrome in the HIV-infected Population
- Highly active antiretroviral therapy (ART) with protease inhibitors (PIs) and nucleoside analogue inhibitors of viral reverse transcriptase (NRTI) allowed a major reduction in the severity and morbidity of HIV infection; however, these drugs were associated with the occurrence of secondary effects collectively termed “ART-related lipodystrophy or metabolic syndrome.”
- Anthrax (also known as Charbon, Milzbrand) is an infectious disease caused by the bacterium Bacillus anthracis.
- Costs of group living include greater energy expenditures, more competition for food, and higher risks of disease