Pericardial Effusion
Before the introduction of HAART, the prevalence of pericardial effusion in asymptomatic AIDS patients was estimated at 11% per year [19]. Although prospective data are lacking, retrospective data suggest that HAART has reduced the overall incidence of pericardial effusion in HIV disease by about 30% [24] (Fig.
7). AIDS patients with pericardial effusion survive a median of 6 months, significantly shorter than do AIDS patients without effusion. Survival is independent of CD4 count and albumin levels [19].A 5-year prospective evaluation of cardiac involvement in AIDS found 16 of 231 patients had or developed pericardial effusions [19]. Three subjects had an effusion on enrollment, and 13 developed effusions during follow-up (12/13 with AIDS at enrollment). Pericardial effusions were generally small (80%) and asymptomatic (87%). The calculated incidence of pericardial effusion among those with AIDS was 11% per year. The prevalence of effusion in AIDS patients may rise over time, reaching an estimated mean of 22% after 25 months of follow-up in asymptomatic patients [19].
Among subjects with AIDS and pericardial effusion, 36% were alive after 6 months of follow-up, whereas 93% of those without effusion were alive at 6 months [19]. Two patients developed pericardial tamponade as assessed by clinical and echocardiographic criteria [19]. Several studies have suggested spontaneous resolution of pericardial effusion over time in 13-42% of affected patients [19]. However, mortality remains markedly increased in patients who had developed an effusion, whether or not the effusion resolved [19].
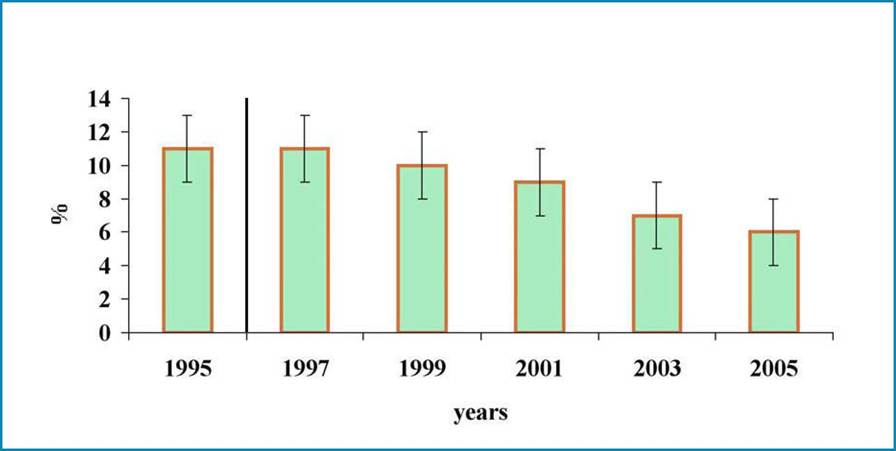
Fig. 7 Prevalence of HIV-associated pericardial effusion in the years 1995-2005. The vertical line indicates the introduction of HAART in the treatment of HIV infection
More on the topic Pericardial Effusion:
- Pericardial Effusion
- Pericardial Effusion and Tamponade
- Pericardial Effusion
- Pericardial Disease
- Pericardial Involvement
- PERICARDITIS
- Pathology of the Pericardium
- Cardiac Tamponade
- Many cardiac complications in acquired immunodeficiency syndrome (AIDS) that may be faced by emergency department (ED) physicians are due to opportunistic infections or malignancy, but they may also be associated with other aspects of human immunodeficiency virus (HIV) disease and its treatment (Table 1) [1].
- Dilated Cardiomyopathy