Infections in Pregnancy
C. David Adair, Shawn P. Stallings, and A. Ben Abdu
Despite numerous advances since the time of Semmelweis when infectious complications were the number one cause of maternal mortality, the obstetric community still faces challenges that remain a major cause of morbidity.
We are reminded, as evident by the recent “swine flu” outbreak, that infections continue to remain a clinical and societal problem. Today, we face “super bug” resistance, increased nosocomial infections, and rapidly declining efficacy of antibiotics. These new challenges for the obstetric caregiver requires continued local surveillance of susceptibilities and resistance, organism identification, and adherence to established evidence based protocols that allow for optimal therapy and minimal contribution to microbiological ecology disruption.URINARY tract infection
Urinary tract infections (UTIs) constitute one of the most common and costly infectious complications of pregnancy, most likely the result of several factors: a relatively short urethra, proximity to the vaginal-anal canal, and physiologic dilatory changes of pregnancy that result in urostasis and reflux. A recent article reported an independent association of maternal UTI with preterm delivery, preeclampsia, intrauterine growth restriction (IUGR), and cesarean delivery (1).
Asymptomatic Bacteriuria
Background
Asymptomatic bacteriuria (ASB) is the presence of bacteria in the urine without concomitant specific urinary tract symptoms. The incidence is not influenced by pregnancy, and the prevalence remains 2% to 7% of all pregnancies, similar to the nonpregnant population, and tends to be more evident in the first trimester (2,3). Certain groups do appear to be at higher risk for ASB. These include patients with lower socioeconomic status, sickle cell trait and disease, diabetes, and chronic urinary retention (2-8).
The American College of Obstetrics and Gynecology (ACOG) recommends routine screening for bacteriuria at the first prenatal visit. Recently, the US Preventive Services Task Force (USPSTF) reaffirmed screening for ASB in pregnant women by urine culture at the first prenatal visit or at 12 to 16 weeks’ gestation (9).Diagnosis
The diagnosis is made by bacterial culture revealing ≥105 organisms of a single species per milliliter of urine without specific UTI symptoms. Because Pyelonephritis may occur with lower colony counts (20k to 50k) in the presence of symptoms or specific isolates such as group B streptococcus or Escherichia coli should be considered positive findings, and patients should be provided treatment based on sensitivity of isolates. A single midstream clean-catch urine culture suffices for the diagnosis. E. coli, Klebsiella, and Enterobacter species account for more than 85% of the isolates. Group B streptococcus, although a rare isolate, when identified in the urine, should be aggressively treated to prevent transmission to the neonate and frank progression to pyelonephritis. This patient will also require intrapartum GBS prophylaxis.
By identifying and treating ASB, a significant reduction in symptomatic infections can be achieved. Left untreated, approximately 40% of all cases of ASB will progress to acute symptomatic infection and 25% to acute pyelonephritis (AP) and its increased attendant morbidity. With adequate therapy, the risk is significantly decreased to only 3% (3,4).
Management
Therapy should be directed by specific isolate identification and sensitivity; some authorities do not recommend C&S evaluation on initial positive cultures in uncomplicated pregnant individuals. Drugs that provide successful ASB treatment and have safe fetal profiles include sulfa-based drugs, first-generation cephalosporins, nitrofurantoin, and penicillin-based alternatives. The latter group should not be used empirically but rather for specific isolates with documented sensitivity because E.
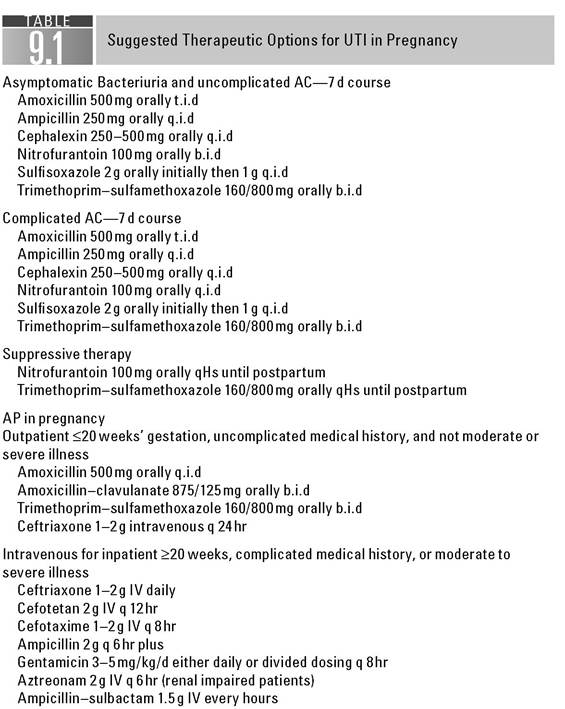
coli has high resistance to penicillin derivatives. It should be remembered that due to increased prevalence of antibiotic resistance the practitioner should use a community accepted first-line agent that presumes adequate coverage and then follow up with specific agents if culture and sensitivity dictates otherwise. In some areas of the country, up to a third of strains have resistance to penicillins and sulfonamides. Nitrofurantoin and trimethop- rim-sulfamethoxazole have geographic resistance rates of 5% to 20%. Typically, in pregnant individuals, single-dose therapy is discouraged. A prolonged course of 7 days is recommended in this population with shorter duration of 3 days being reserved for nonpregnant patients. Suggested drug regimens are presented in Table 9.1. After completion of treatment, a test of cure culture should be obtained, because as many as one third of patients will have persistent bacteriu- ria. When persistence is confirmed, longer courses and/or suppressive therapy may be prudent.Acute Cystitis
Acute cystitis (AC) complicates 0.3% to 1.3% of all pregnancies. One third of the cases represent progression from ASB, and the remainder represent de novo infection and recurrence can be up to 1.3% (8). Patients with AC often present in the second trimester with complaints of urgency, frequency, dysuria, and pelvic pressure discomfort. A lower colony count (i.e., ≥102) in the presence of the symptoms is usually sufficient to confirm diagnosis. In general, the same isolates as found in ASB are the culprits in AC such as E. coli, Gram-negative facultative organisms, Group B Streptococcus (GBS), and Staphylococcus saprophyticus. Therapy is largely empiric at first, then it is directed to specific agents as culture and sensitivities of isolates become available. Appropriate first-line therapies include nitrofurantoin macrocrystals or first-generation cephalposporins. Therapeutic options are included in Table 9.1. Symptomatic abatement should occur between 48 and 72 hours, and the absence of symptom resolution should prompt reevaluation.
Efficacy of therapy should be confirmed by conductance of a test of cure. From 17% to 25% of pregnant patients with AC experience a recurrent bout of AC or other UTI during pregnancy; importantly, AC does not increase the incidence of adverse pregnancy outcome like some of its counterparts (8).Acute Pyelonephritis
Background
AP disorder complicates more than 1% to 2.5% of all pregnancies (10). Forty percent of pregnant women with AP have antecedent symptoms of lower UTI. Unlike
ASB and AC, pregnancy does seem to predispose to AP. Two thirds of cases arise in women with previously documented positive urine culture results and the remainder arise de novo. Most cases of AP in pregnant women occur in the second and third trimesters when significant and maximal physiologic changes have occurred (4,10). The disease is thought to result from the significant physiologic changes of the genitourinary system, namely, urethral dilation, mechanical obstruction of the gravid uterus, and significant glucosuria and aminoaciduria.
Diagnosis
The diagnosis of AP is based on the presence of systemic signs and symptoms that include fever, chills, nausea, vomiting, and costovertebral angle tenderness. Almost always, these cases are complicated by a fever and, in some cases, significant temperature elevation may occur ≥44°C (11). Costovertebral sensitivity tends to be right sided in the predominance of cases but does not exclude the possibility of bilateral or left-sided tenderness.
Laboratory findings usually include an elevated white blood cell count, but occasionally, in mild or early infections, this may be normal. Some investigators have reported decreased hematocrit and transient renal dysfunction (10,12). Significant pyuria, hematuria, and ultimately positive urine cultures are mainstay findings. It is not unusual for a patient to have “sterile” urine despite having classic symptoms.
When confronted with this clinical scenario, treatment should not be postponed.Effects ofAP are not limited to the kidney. These include hemolytic anemia, renal dysfunction, and pulmonary dysfunction including transient mild distress to frank adult respiratory distress syndrome (13,14). About 15% to 20% of women with AP also have bacteremia (2). As with any systemic infection combining with the immunocompromised status of pregnancy, septic shock may result. Unlike ASB and AC, AP is associated with increased occurrence of uterine contractions and preterm labor.
Management
The treatment of pyelonephritis consists of aggressive systemic intravenous antibiotics and judicious fluid management. All pregnant patients suspected of having pyelonephritis should be admitted to the hospital for treatment. The i ni- tial antimicrobial selection should be reflective of most common isolates and should be cost sensitive. Several regimens can be employed. These include gentamicin and ampicillin or first- or third-generation cephalosporins. A randomized controlled trial showed 95% efficacy of these regimens (15). This selection of the third-generation cephalosporins allows for the possibility of early discharge and outpatient therapy in gestations Maternal mortality is fortunately a rare event. Neonatal morbidity can be significant and can lead to neonatal death. Neonates whose intrapartum course is complicated by IAI are at significantly increased risks of sepsis, congenital pneumonia, and cerebral palsy (26,27).
Numerous risk factors for the development of IAI have been elucidated. These include preterm labor, preterm rupture of membranes, dysfunctional labor, prolonged rupture of term membranes (>18 hours), meconium-stained amniotic fluid, presence of cervical pathogens, bacterial vaginosis, number of vaginal examinations, and presence of intrauterine fetal monitoring and contractile monitors (20,28-40). IAI most commonly is caused by bacteria found in the lower genital tract and is polymicrobial rather than related to a single pathologic isolate.
The two most common isolates are group B streptococcus and E. coli.Management
The treatment of IAI is approached best by preventive measures, for example, by avoiding numerous or unnecessary vaginal examinations and intrauterine monitoring and by identifying and treating cervical pathogens before intrapartum presentation. When prevention proves inadequate, systemic antibiotic administration is required. Withholding antibiotics until after delivery is not prudent. IAI complicates both the maternal and the neonatal units. Thus, antibiotic selection and administration should be considered therapy for both the mother and the fetus. The selection should cover usual vaginal borne pathogens, especially group B streptococcus and enteric organisms. Although IAI alone is not an indication for cesarean delivery, when c-section is required in the face of IAI, coverage should also include antimicrobial activity directed to anaerobes.
Even though risk factors and common isolate epidemiology are well-known, the optimal “gold standard” therapy remains less well defined. Historically, penicillin or ampicillin, paired with the aminoglycoside gentamicin, has been favored. Single broad-spectrum therapeutic agents have also been advocated. The selection is empiric and should be broad enough to cover usual suspected pathogens (20-23).
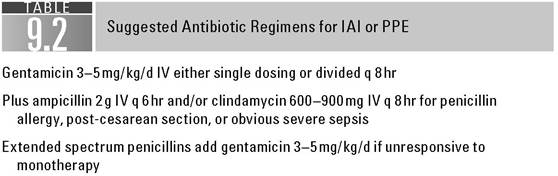
Some commonly recommended drug regimens in the treatment of IAI are presented in Table 9.2. Again, IAI is not in and of itself an indication for cesarean delivery, but rather the mode of delivery should follow standard obstetric guidelines. With close fetal monitoring and the provision of good antibiotic coverage, no particular “rush” for delivery is indicated. There is accumulating evidence that respiratory distress syndrome, periventricular leukomalacia, and cerebral palsy are increased in both term and preterm infants. A thorough discussion of this is beyond the scope of this text. Once delivery has occurred, the decision to continue antibiotics postpartum remains controversial. One reasonable approach is to continue antibiotics in the presence of a cesarean delivery or for the patient who appears clinically ill. Otherwise, antibiotic discontinuance and close observation are practical (24).
POSTPARTUM ENDOMETRITIS
Background
Postpartum endometritis (PPE) complicates 1% to 3% of all vaginal deliveries and is much more frequent following cesarean delivery (41-43). This wide range of incidence depends on socioeconomic, delivery route, and labor parameters. PPE can be a continuation of IAI or arise de novo. The microbiologic isolates, like for IAI, the infection tends to be polymicrobial rather arising from a specific species. A mixed aerobic-anaerobic population is expected, especially after cesarean delivery (43,44). Single-species PPE should be suspected when the patient has received the benefit of prophylactic antibiotics (45-48).
Diagnosis
PPE is diagnosed in the patient with fever ≥38°C, uterine tenderness, foulsmelling lochia, abdominal pain, leukocytosis, and, most importantly, the absence of other discernible causes of infection (e.g., pyelonephritis or pneumonia). Some cases of IAI, without question, are severe enough that despite delivery of the infected placenta or membrane, persistent infection accompanies the puerperium, particularly in cases complicated by cesarean delivery. In those cases, antibiotic administration should be extended into the puerperium. However, in the patient with low-grade IAI or suspected de novo PPE, a clinical examination and evaluation are mandatory. The temptation to empirically administer antibiotics should be restrained until the diagnosis is firmly established.
Clinical risk factors parallel those of IAI. Chiefly, the factors include the duration of membrane rupture and labor, internal monitoring, numerous vaginal examinations, cesarean delivery, IAI, lower socioeconomic status, and the presence of meconium staining (49-62).
Management
The evaluation of the patient includes a detailed history and review of the labor record to ascertain the presence of risk factors and whether the patient has mitigating circumstances, such as antibiotic prophylaxis, immunosuppressive disorders, and drugs. A physical examination should exclude other likely sources. Most cases of endometritis are relatively straightforward in diagnosis; occasionally, the clinician encounters a postpartum fever with absent pinpoint focal findings. After thorough evaluation is inconclusive, it is reasonable to provide supportive measures, that is, antipyretics, and to observe the non- ill-appearing patient. However, if the patient’s temperature is ≥38°C, particularly when following a cesarean delivery, antibiotics are generally indicated.
Antibiotic selection should be broad enough to cover all of the usual pathogens and should be aimed at a polymicrobial infection. Several recommended regimens are presented in Table 9.2. With appropriate selection, clinical symptoms and fever begin to abate in 24 to 48 hours. Blood cultures are generally reserved for patients with complicated underlying medical conditions or very ill appearing. For those with relatively straight forward PPE, omission of blood culture is acceptable. Failure to respond by 72 hours should prompt a reevaluation of the patient and antibiotic coverage to ensure no existence of a therapeutic gap in the chemotherapy. Pelvic ultrasound or computed tomography (CT) scan may assist in identifying hematoma, abscess, and retained placental products or instruments and in excluding septic pelvic thrombophlebitis.
If a hematoma is identified, CT-guided drainage may be beneficial. When septic pelvic thrombophlebitis is present, intravenous heparinization therapy for 7 days is recommended. When confronted with a pelvic abscess, unresponsive to antibiotics and nonamenable to needle drainage, surgical intervention is required. The surgical approach must be aggressive, because, left unchecked, the abscess may lead to myonecrosis and subsequent death.
Preventive measures to diminish PPE include several modalities. The foremost example is that of prophylactic antibiotic administration at the time of the cesarean delivery. Usually, a first-generation cephalosporin such as cefazolin is administered at the time of the cord clamping or in some series administered within 1 hour of surgical incision. For true allergic response to penicillins, those individuals are generally recommended to be treated with both gentamicin and clindamycin. Amnioinfusion has been suggested to reduce PPE in patients undergoing cesarean delivery with clear amniotic fluid and membrane rupture of >6 hours’ duration (63,64), although this is not universally embraced. This approach seems to be not beneficial in cases with meconium staining (65).
PPE is more common after cesarean delivery than vaginal delivery. Because of the increased cesarean rates, PPE has become one of the most common causes of maternal morbidity. However, the use of single-dose perioperative antibiotic prophylaxis is likely the single greatest intervention to reduce the rates of postcesarean pelvic infections in the past 25 years (66). Prevention is the most prudent approach to PPE morbidity. However, when simple measures fail and active infection occurs, aggressive therapy aimed at the most common isolates is indicated. The clinician should be cognizant of the polymicrobial nature of PPE and, if therapy becomes unresponsive, more serious etiologies should be considered.
HERPES INFECTION
Herpes simplex virus (HSV), cytomegalovirus (CMV), and varicella are specific viral pathogens that all belong to the family Herpesidae, all contain doublestranded DNA, and all have significant adverse maternal and fetal/neonate effects.
Herpes Simplex Virus
Background
HSV-1 and -2 serotypes invade neural roots through mucosal membrane defects. Infection may be primary or, after acquisition, may remain dormant with recurrent episodic outbreaks. Acquisition can be by genital:genital, oral:genital, or anal:genital sexual contact. Serotypes previously were site specific, but each serotype may be associated with acute or recurrent HSV infection at oral, genital, or nongential sites. However, HSV-2 is more likely to be associated with recurrence regardless of site selection (67-69). Approximately 45 million adolescent and adult Americans are infected with HSV (70). Therefore, it may be a frequently encountered issue to be addressed in the pregnant female.
Diagnosis
The diagnosis of HSV infection is largely clinical. A history of vesicular, painful, burning ulcers prompts the decision to seek medical evaluation. During this evaluation, the clinician should attempt to distinguish primary from recurrent HSV infection. Primary HSV acquisition is associated with flulike symptoms, lymphadenopathy, fever, and malaise. These viral syndrome symptoms typically are absent with recurrent HSV flare-ups. Exposure to onset of viral disease is >2 to 7 days (67,71).
Viral culture may be of assistance in providing absolute confirmation. However, clinically, if primary HSV infection is suspected, therapy should not be withheld pending culture results. Serum immunoglobulin M (IgM) and IgG antibodies may be of assistance in confirming the absence of previous infection. Papanicolaou smear test and Tzanck test have also been used to suggest HSV infection by identification of viral cytologic effects, but they lack sensitivity to be used for routine clinical care.
Recent evidence has suggested important prognostic values of primary versus recurrent HSV infection in pregnancy. Pregnancy per se does not influence the course of HSV infection, either in primary or recurrent episodes; however, both may result in hepatitis, meningitis, or pneumonia. Systemic manifestations require prolonged intravenous therapy with acyclovir. Disseminated HSV infection is associated with increased risk of maternal and neonatal mortality.
Neonatal vertical transmission remains the paramount concern for HSV infection complicating pregnancy. Most significant neurologic and severe adverse outcomes develop in those neonates with infection at or near the time of maternal primary disease, whereas infants born to mothers with recurrent disease have the least chance of acquisition and less morbidity (72).
Management
Obstetric management remains supportive and directed to symptomatic management. The clinician should counsel women on possible transmission to partners and screen for other sexually transmitted diseases. Cesarean delivery is necessary for the patient in labor who has active disease or has the prodromal symptoms in cases of known recurrence. Cesarean delivery will not necessarily provide 100% prevention of HSV transmission to the neonate. Approximately 25% of affected neonatal cases were delivered by cesarean delivery (67,73,74). Vertical transmission rates are 30% to 60% when there is a primary HSV outbreak at the time of delivery (75). The rates are 3% if having a recurrent genital outbreak at the time of delivery, and only 2 per 10,000 in a patient with a history of HSV but no active lesions at the time of delivery (76).
There is currently no universally accepted screening guideline for HSV in pregnancy. Therapy is with any of the synthetic acyclic purine nucleoside analogues such as acyclovir, valacyclovir, and famciclovir. These agents (Category B) have no evidence of teratogenic or adverse effects on the human fetus. They should be used in doses similar to those used in a nonpregnant patient. Prophylactic suppression has been reputed to be successful in reducing recurrence of HSV infection at term. Generally, prophylaxis is initiated at 36 weeks (77,78). ACOG currently recommends offering suppressive viral therapy for women with active recurrent genital herpes at or beyond 36 weeks’ gestation (79). However, a recent Cochrane review suggests that the overall risk of neonatal herpes is low, and there is insufficient evidence to determine if antiviral prophylaxis reduces the incidence of neonatal herpes (80).
Cytomegalovirus
Background
CMV is the most common perinatally transmitted viral infection, occurring in 1% to 2% of all neonates. Like HSV, it can be transmitted to the fetus by either primary or reactivation of CMV infection. More than 85% of patients in low socioeconomic status have evidence ofprevious CMV infection and about 50% of the adult sexually active population. Fetal transmission in these cases is is fairly straightforward. Most patients have a history of recent exposure of acute vesicular maculopapular rash of the scalp and trunk with progression to the extremities and other body areas. These lesions are commonly accompanied by flulike symptoms, myalgia, headaches, and fever. Each new lesion has active viral shedding for 6 days with “crusting” persisting for 1 week. Fever generally persists until cessation of lesion formation.
VZ infection usually is self-limiting and treatment is thus largely symptomatic. VZ infection complicating pregnancy, however, presents unique challenges to the clinician. Complications are usually more frequent and severe when accompanying pregnancy. These include meningitis, encephalitis, arthritis, acute glomerulonephritis, and pneumonia. Pneumonia is the most frequent complication and is of the most concern. Varicella pneumonia may result in respiratory insufficiency, edema emphysema, superimposed bacterial infections, and even death. Pulmonary insult and injury lead to maternal and fetal hypoxia.
Varicella has been associated with an embryopathy (91). However, no increased adverse perinatal outcome has been reported, such as spontaneous abortion, prematurity, growth restriction, or death (92-95). The embryopathy syndrome was originally described by LaForest and Lynch (91). Characteristics are skin scarring, limb hypoplasia, and CNS and eye abnormalities. Developmental abnormalities appear to be limited to exposure at 12 weeks or less and occur in 2% to 3% of pregnancies.
The risk of congenital anomalies occurring secondary to varicella has been estimated to be approximately 2% (94-99). These anomalies include cicatrix skin deformities, ocular scarring, cataracts, chorioretinitis, and limb shortening (91,93,96,100-102).
The exposure to varicella requires documenting the antibody status of women who have uncertain varicella history. The majority of women who have no prior history of varicella infection will have serologic evidence of varicella exposure and IgG conversion. The patient who has negative IgG titers should receive VZ immunoglobulin (VZIG). The dose is 125 units∕10kg intramuscularly with a maximum of 625 units or five vials intramuscularly and is ideally administered within 96 hours of exposure. Once varicella infection is established, care is directed at symptomatic relief, prevention of community spread, especially to other pregnant women, and close surveillance for complications of disease progression. Acyclovir can be used to provide some symptom relief in mild to moderate cases, although this is largely an empiric treatment. Cases of severe disease of pneumonia mandates intravenous acyclovir at 10mg∕kg administered every 8 hours. The patient with any pulmonary complaint should be given acyclovir and observed closely in a negative airflow room.
Labor, whether it is preterm or term, frequently accompanies severe varicella infection. Caution should be used in administering tocolytics and glucocorticosteroids. Maternal viremia results in antibody production within 4 to 5 days of rash development. Thus, the infant at highest risk of neonatal varicella acquisition is born within 2 to 5 days of rash development. If labor begins during this interval, consideration of tocolysis may be prudent until 5 days after the appearance of the rash, even in term fetuses. Neonates born during this time interval have the highest risk of adverse complication and should therefore receive VZIG and acyclovir (92,103,104). Of interest is the increasing number of varicella vaccinated females that are approaching reproductive age and how the vaccine will impact varicella in pregnancy.
References
1. Mazo-Dray E, Levy A, Schlaeffer F, Sheiner E. Maternal UTI: is it independently associated with adverse pregnancy outcome? JMatern Fetal Noenatal Med. 2009;22(2): 124-128.
2. Creasy RK, Resnik R, Iams JD, Lockwood CJ, Moore TR. Maternal and fetal infections. In: Creasy and Resniks Maternal Fetal Medicine. 6th Ed. St. Louis, MO: Saunders- Elsevier,2009.
3. Whalley; P. Bacteriuria of pregnancy. Am J Obstet Gynecol. 1967;97:732.
4. Turck M, GoffBS, Petersdorf RG. Bacteriuria in pregnancy: relation to socioeconomic factors. N Engl JMed. 1962;266:857.
5. Whalley PJ, Mrtin RG, Pritchard JA. Sickle cell trait and urinary tract infection duringpregnancy. JAMA. 1964;189:9036.
6. Baker ER, Cardenas DD, Benedetti TJ. Risks associated with pregnancy in spinal cord-injured women. Obstet Gynecol. 1992;80:4258.
7. Lye WC, Chan RK, Lee EJ, et al. Urinary tract infections in patient with diabetes mellitus. J Infect. 1992;24:16974.
8. Harris RE, Gilstrap LC. Cystitis during pregnancy: a distinct clinical entity. Obstet Gynecol. 1981;57:578-580.
9. USPSTF. Ann Intern Med. 2008;149(1):43-47.
10. Gilstrap LC, Cunningham FG, Whalley PJ. Acute pyelonephritis in pregnancy: an anterospective study. Obstet Gynecol. 1981;57:409-413.
11. Stenqvist K, Standberg A, Lidin-Janson G, et al. Virulence factors of Escherichia coli in urinary isolates from pregnant women. JInfect Dis. 1987;156:870-877.
12. Whalley PJ, Cunningham FG, Martin FG. Transient renal dysfunction associated with acute pyelonephritis of pregnancy. Obstet Gynecol. 1974;46:17-47.
13. Cunningham FG, Lucas MJ, Hankins GDV. Pulmonary injury complicating antepartum pyelonephritis. Am J Obstet Gynecol 1987;156:797-807.
14. Cunningham FG, Leveno KJ, Hankins GDV, et al. Respiratory insufficiency associated with pyelonephritis during pregnancy. Obstet Gynecol. 1984;63:12-15.
15. Wing DA, Hendershott CM, Debesque L, et al. A randomized controlled trial of three antibiotic regimens for the treatment of pyelonephritis in pregnancy. Am J Obstet Gynecol. 1998;92:249.
16. Millar LK, Wing DA, Paul RH, et al. Outpatient treatment of pyelonephritis in pregnancy: a randomized controlled trial. Obstet Gynecol. 1995;86:560-564.
17. Sanchez-Ramos L, McAlpine KJ, Adair CD, et al. Pyelonephritis in pregnancy: once- a-day ceftriaxone versus multiple dose cefazolin: a randomized, double-blind trial. Am J Obstet Gynecol. 1995;172:129-133.
18. Zinner SH, Kass EH. Long-term (10-14 years) follow-up of bacteriuria of pregnancy. N Engl JMed. 1971;285:820-822.
19. Koh Ke, Chan FH, Monfared AH, et al. The changing perinatal and maternal outcome in chorioamnionitis. Obstet Gynecol. 1979;53:730.
20. Gibbs RS, Castillo MS, Rogers PJ. Management of acute chorioamnionitis. Obstet Gynecol. 1980;136:709.
21. Hauth JC, Gilstrap LC III, Hankins GDV, et al. Term maternal and neonatal complications of acute chorioamnionitis. Obstet Gynecol. 1985;66:59.
22. Gilstrap LC III, Leveno KJ, Cox SM, et al. Intrapartum treatment of acute chorioamnionitis: impact on neonatal sepsis. Am J Obstet Gynecol. 1988;159:579.
23. Satin AJ, Maberry MC, Leveno KJ, et al. Chorioamnionitis: a harbinger of dystocia. Obstet Gynecol. 1992;79:91-93.
24. Wendel PJ, Cox SM, Roberts SW, et al. Chorioamnionitis: association of nonreassuring fetal heart rate patterns and interval from diagnosis to delivery on neonatal outcome. Infect Dis Obstet Gynecol. 1994;2:162.
25. Gibbs RS, SuffP. Progress in pathogenesis and management of clinical intraamniotic infection. Am J Obstet Gynecol. 1991;164:1317.
26. Duff P, Sanders R, Gibbs RS. The course of labor in term pregnancies with chorioamnionitis. Am J Obstet Gynecol. 1983;147:391.
27. Yoon BH, Romero R, Kim CJ, et al. High expression of tumor necrosis factor-alpha and interleukin-6 in periventricular leukomalacia. Am J Obstet Gynecol. 1997;177: 406-411.
28. Newton ER. Chorioamnionitis and intraamniotic infection. Clin Obstet Gynecol. 1993; 36:795.
2J9D., LHoaogffer WD. Management of chorioamnionitis. Surg Gynecol Obstet. 1984;
158:161.
30. Guzick DS, Winn K. The associate of chorioamnionitis with preterm delivery. Obstet Gynecol. 1985;65:11.
31. Sturchier D, Menegaz F, Dialing J. Reproductive history and intrapartum fever. Gynecol Obstet Invest. 1986;21:182.
32. Newton ER, Prihoda TJ, Gibbs RS. Logistic regression analysis of risk factors for intra-amniotic infection. Obstet Gynecol. 1989;73:571.
33. Soper DE, Mayall CG, Dalton HP. Risk factors for intraamniotic infection: a prospective epidemiologic study. Am J Obstet Gynecol. 1989;161:562.
34. Edwards LA, Barrada MI, Hamann AA, et al. Gonorrhea in pregnancy. Am J Obstet Gynecol. 1978;132:637.
35. Regan JA, Chao SJ, James SL. Premature rupture of the membranes, preterm delivery and group B streptococcal colonization of mother. Am J Obstet Gynecol. 1981; 141:184.
36. Hillier S, Krohn MA, Kiviat NB, et al. Microbiologic causes and neonatal outcomes associated with chorioamnion infection. Am J Obstet Gynecol. 1991;165:955.
37. Gibbs RS. Chorioamnionitis and bacterial vaginosis. Am J Obstet Gynecol. 1993; 169:460.
38. Romero R, Hanaoka S, Mazor M, et al. Meconium-stained amniotic fluid: a risk factor for microbial invasion of the amniotic cavity. Am J Obstet Gynecol. 1991;164:859.
39. Adair CD, Ernest JM, Sanchez-Ramos L, et al. Meconium-stained amniotic fluid- associated infectious morbidity: a randomized double-blind trial of ampicillinsulbactam prophylaxis. Obstet Gynecol. 1996;88:216.
40. Piper Jm, Newton ER, Berkus MD, et al. Meconium: a marker for peripartum infection. Obstet Gynecol. 1998;91:741.
41. Gilstrap LC III, Cunningham FG. The bacterial pathogenesis of infection following cesarean section. Obstet Gynecol. 1979;53:545-549.
42. Sweet RL, Ledger WJ. Cefoxitin: single agent treatment of aerobic-anaerobic pelvic infections. Obstet Gynecol. 1979;54:193-198.
43. Gibbs RS. Clinical risk factors for puerperal infection. Obstet Gynecol. 1980;55(s): 178-183.
44. Phillips LE, Faro S, Martens MG, et al. Post cesarean microbiology of high-risk patients treated for endometritis. Curr TherRes. 1987;42:1157-1165.
45. Faro S, Cox SM, Phillips LM, et al. Influence of antibiotic prophylaxis on vaginal microflora. Am J Obstet Gynecol. 1986;6(S):54-56.
46. Stever HG, Forward KR, Tynell DC, et al. Comparative cervical flora-microflora shift after cefoxitin or cefazolin prophylaxis against infection following cesarean section. Am J Obstet Gynecol. 1984;149:718-721.
47. Gilstrap LC III. Puerperal infection. In: Faro S, ed. Diagnosis and Management of Female Pelvic Infection in PrimaryCare Medicine. Baltimore, MD: Williams & Wilkins; 1985:151-167.
48. Gilstrap LC III. Prophylactic antibiotics for cesarean section and surgical procedures. J Rep Med. 1988;33:588-590.
49. Gibbs RS, Castillo MS, Rogers PJ. Management of acute chorioamnionitis. Obstet Gynecol. 1980;136:709-713.
50. Newton ER. Chorioamnionitis and intraamniotic infection. Clin Obstet Gynecol. 1993; 36:795.
51. Looff JD, Hager WD. Management of chorioamnionitis. Surg Gynecol Obstet. 1984; 158:161.
52. Guzick DS, Winn K. The associate of chorioamnionitis with preterm delivery. Obstet Gynecol. 1985;65:11.
53. Sturchler D, Menegaz F, Dialing J. Reproductive history and intrapartum fever. Gynecol Obstet Invest. 1986;21:182.
54. Newton ER, Prihoda TJ, Gibbs RS. Logistic regression analysis of risk factors for intra-amniotic infection. Obstet Gynecol. 1989;73:571.
55. Soper DE, Mayall CG, Dalton HP. Risk factors for intraamniotic infection: a prospective epidemiologic study. Am J Obstet Gynecol. 1989;161:562.
56. Edwards LA, Barrada ML, Hamann AA, et al. Gonorrhea in pregnancy. Am J Obstet Gynecol. 1978;132:637.
57. Regan JA, Chao SJ, James SL. Premature rupture of the membranes, preterm delivery and group B streptococcal colonization of mother. Am J Obstet Gynecol. 1981; 141:184.
58. Hillier S, Krohn MA, Kiviat NB, et al. Microbiologic cases and neonatal outcomes associated with chorioamnion infection. Am J Obstet Gynecol. 1991;165:955.
59. Gibbs RS. Chorioamnionitis and bacterial vaginosis. Am J Obstet Gynecol. 1993; 169:460.
60. Romero R, Hanaoka S, Mazor M, et al. Meconium-stained amniotic fluid: a risk factor for microbial invasion of the amniotic cavity. Am J Obstet Gynecol. 1991;164:859.
61. Adair CD, Ernest JM, Sanchez-Ramos L, et al. Meconium-stained amniotic fluid-associated infectious morbidity: a randomized double-blind trial of ampicillin- sulbactamprophylaxis. Obstet Gynecol. 1996;88:216.
62. Piper JM, Newton ER, Berkus MD, et al. Meconium: a marker for peripartum infection. Obstet Gynecol. 1998;91:741.
63. Moen MD, Besinger RE, Tomich PG, et al. Effect of amnioinfusion of the incidence of postpartum endometritis in patients undergoing cesarean delivery. J Reprod Med. 1995;40:383-386.
64. Monahan E, Katz VL, Cox RL. Amnioinfusion for preventing puerperal infection: a prospective study. J Reprod Med. 1995;40:721-723.
65. Adair CD, Weeks JW, Johnson G, et al. The utility of amnioinfusion in the prophylaxis of meconium-stained amniotic fluid infectious morbidity. Infect Dis Obstet Gynecol. 1997;5:366-369.
66. Cunningham FG, Leveno KJ, Bloom SL, et al. Puerperal infection. In: Williams Obstetrics. 22nd Ed. New York, NY: McGraw-Hill; 2005.
67. Cook CR, Gall SA. Herpes in pregnancy. InfectDis Obstet Gynecol. 1994;1:298-304.
68. Reeves W, Corey L, Adams H, et al. Risk of recurrence after first episodes of genital herpes. N Engl JMed. 1981;305:315-319.
69. Corey L, Adams H, Brown Z, et al. Genital herpes simplex virus infections: clinical manifestation, course and complications. Ann Intern Med. 1983;98:958-972.
70. Fleming DT, McQuillan GM, Johnson RE, Nahamias AJ, Aral SO, Lee FK. Herpes simplex virus type 2 in the United States, 1976 to 1994. N Engl J Med. 1997;337: 1105-1111.
71. Maccato M. Herpes in pregnancy. Clin Obstet Gynecol. 1993;36:869-877.
72. Brown ZA, Selke S, Zeh J, et al. The acquisition of herpes simplex virus during pregnancy. N Engl JMed. 1997;337:509-515.
73. Whitley R, Corey L, Arvin A, et al. Changing presentation of herpes simplex virus infection in neonates. J Infect Dis. 1988;158:109-116.
74. Stone KM, Brooks CA, Guinan ME, et al. National surveillance for neonatal herpes simplex virus infections Sex Transm Dis. 1989;16:152-156.
75. Brown ZA, Selke S, Zeh J, et al. The acquisition of herpes simplex virus during pregnancy. NEngl JMed. 1997;337:509-515.
76. Brown ZA, Benedetti J, Ashley R, et al. Neonatal herpes simplex virus infection in relation to asymptomatic maternal infection at time of labor. N Engl JMed. 1991; 324:1247-1252.
77. Burroughs Wellcome Company. Pregnancy outcomes following systemic prenatal acyclovir exposure.June 1, 1984 to June 30, 1993. Morbid Mortal Wkly Rep. 1993;42: 806-809.
78. ScoffLL, Sanchez PJ, Jackson GL, et al. Acyclovir suppression to prevent cesarean section after first episode genital herpes in pregnancy. Obstet Gynecol. 1996;87:69-73.
79. Managing Herpes in Pregnancy. ACOG Practice Bulletin. No. 82, June 2007.
80. Hollier LM, Wendel GD. Third trimester antiviral prophylaxis for preventing maternal genital herpes simplex virus recurrences and neonatal infection. Cochrane Database Syst Rev. 2008;1:CD004946.
81. Stagno S, Whitely RJ. Herpes virus infection of pregnancy, Part 1. Cytomegalovirus and Epstein-Barr virus infection. N Engl JMed. 1986;313:1270-1274.
82. Raynor BD. Cytomegalovirus infection in pregnancy. Semin Perinatol. 1993;17:394-402.
83. Sison AV, Sever JL. Cytomegalovirus infections in pregnancy. In: Queenan JT, ed. Management of High Risk Pregnancy. Boston, MA: Blackwell Scientific Publications; 1994:315-321.
84. Donner C, Liesnard C, Content J, et al. Prenatal diagnosis of 52 pregnancies at risk for congenital cytomegalovirus infection. Obstet Gynecol. 1993;82:481-486.
85. Dong W, Yan C, Yi W, et al. detection of congenital cytomegalovirus infection by using chorionic villi of the early pregnancy and polymerase chain reaction. Int J Gynecol Obstet. 1994;44:229-231.
86. Catanzaarite V, Dankner WM. Prenatal diagnosis of congenital cytomegalovirus infection: false negative amniocentesis at 20 weeks' gestation. Prenat Diagn. 1993;12: 1021-1125.
87. Hogge WA, Buffone GJ, Hogge JS. Prenatal diagnosis of cytomegalovirus (CMV) infection: a preliminary report. Prenat Diagn. 1993;13:131-136.
88. Twickler DM, Perlman J, Maberry MC. Congenital cytomegalovirus infection presenting as cerebral Ventriculomegaly on antenatal sonography. Am J Perinatol. 1993;10:404-406.
89. Nigro G, Adaler SP, LaRorre R, et al. Passive immunization during pregnancy for congenital cytomegalovirus infection. NEnglJMed. 2005;353:1350-1362.
90. Stagno S, Whitely RJ. Herpes virus infection of pregnancy. Part II. Herpes simplex virus varicella-zoster virus infections. N EnglJMed. 1985;313:1327-1332.
91. LaForest E, Lynch CL. Multiple congenital defects following maternal varicella. N EnglJMed. 1947;126:534-537.
92. Brunell PA. Varicella zoster-infections. In: Amstey MS, ed. Virus Infection in Pregnancy. Orlando, FL: Grune & Stratton; 1984:131-145.
93. Paryani SG, Arvin AM. Intrauterine infection with varicella-zoster virus after maternal varicella. N Engl JMed. 1986;314:1542-1546.
94. Preblud S, Cochi S, Orenstein W. Varicella-zoster infection in pregnancy. N Engl J Med. 1986;315:14-15.
95. Enders G. Varicella-zoster virus infection in pregnancy. Prog Med Virol. 1984;29: 166.
96. Srabstein JC, Morris N, Larke RP, et al. Is there a congenital varicella syndrome? J Pediatr. 1974;84:239-243.
97. Siegal M, Fuerst HT. Low birth weight and maternal viral diseases: a prospective study of rubella, measles, mumps, chicken pox, and hepatitis. JAMA. 1966;197:88.
98. Seigel M, Fuerst HT, Pareso NS. Comparative mortality in maternal virus diseases: A prospective study on rubella, measles, mumps, chicken pox, and hepatitis. N Engl JMed. 1966;274:76-78.
99. Fox MJ, Krumpiegel ER, Teresi JL. Maternal measles, mumps, and chicken pox as a cause of congenital anomalies. Lancet. 1972;2:62-69.
100. McKendryJBJ, Bailey JD. Congenital varicella associated with multiple defects. Can MedAssoc J. 1977;108:66-67.
101. Charles NC, Bennett TW, Margolis S. Ocular pathology of the congenital varicella syndrome. Arch Ophthalmol. 1977;95:2034-2037.
102. Coftier E. Congenital varicella cataract. Am J Ophthalmol. 1978;86:627.
103. Raine DN. Varicella infection contracted in utero: sex incidence and incubation period. Am J Obstet Gynecol. 1966;94:1144-1145.
104. Steen J, Pederson RB. Varicella in a newborn girl. J Oslo City Hosp. 1959;9:36-45.
More on the topic Infections in Pregnancy:
- Infections in Pregnancy
- Human Immunodeficiency Virus (HIV) Infection and Pregnancy: Labor and Delivery Management
- 24 HIV in Pregnancy
- Pneumonia
- 11 Perinatal Infections
- Chapter 8 Maternal medicine and infections
- Intra-amniotic infection, meconium staining of the amniotic fluid, and meconium aspiration syndrome: what is the link?
- Detailed contents
- Miscarriage
- Chapter 5 Normal pregnancy