Encephalitozoon cuniculi Infection: Encephalitozoonosis; Microsporidiosis
“Infectious motor paralysis” attributed to a “protozoan parasite” was first reported in laboratory rabbits by Wright and Craighead in 1922. Encephalitozoon cuniculi is an obligate intracellular microsporidian that infects a variety of mammalian hosts, and very commonly infects the domestic rabbit.
Because of its wide host range, humans are susceptible to zoonotic infection, and severe disease has been observed in immunosuppressed individuals. Taxonomists have historically disagreed on the classification for the organism, but genomic sequencing has now confirmed that E. cuniculi is a eukaryotic fungus within the phylum microsporidia. Gene sequencing among strains originating from different host species indicates identical gene content, but marked intraspecies genetic diversity. The prevalence of seropositive animals in some conventional rabbit populations is high, as well as among pet and wild rabbits. The organism is characterized by the presence of a coiled polar filament in the mature spore stage. Following the extrusion of the spor- oplasm from the spore coat, the sporoplasm may then invade a susceptible host cell. Penetration may be due to the mechanical forces exerted by the extruded polar filament or due to an active migratory process by the sporoplasm. Following entry into the cell, multiplication occurs in association with a cytoplasmic vacuole. Sporoblasts develop into mature spores, and finally the cell ruptures, releasing organisms that can then repeat the cycle.Epizootiology and Pathogenesis
Transmission occurs through organisms excreted in the urine, as well as transplacentally. Rabbits are readily infected experimentally by the oral or respiratory route, and iatrogenic transmission through contaminated needles may also occur. Following ingestion/oral inoculation, spores appear to pass via infected mononuclear cells into the systemic circulation.
Initially, target organs are those of high blood flow, such as lung, liver, and kidney. In rabbits inoculated orally with E. cuniculi and examined at 31 days postinoculation, moderate to marked lesions were demonstrated primarily in the lung, liver, and kidney, and occasionally in the myocardium. No lesions were present in the central nervous system at 1 month. At 3 months, moderate to severe lesions were evident histologically in the kidney, and changes were minimal in the lung, liver, and heart, but lesions were evident in the brain at this stage. Serum antibody titers may be detectable by 3-4 weeks and reach high titers by 6-9 weeks. Spores have been seen in the urine at 1 month and may be excreted in large numbers up to 2 months. Only small numbers are excreted thereafter. Shedding of spores is essentially terminated by 3 months. Spores survive for less than 1 week at 4°C but may remain viable for at least 6 weeks at 22°C.Pathology
Infection is frequently subclinical, but rabbits may present with a variety of neurologic signs, including head tilt, ataxia, vestibular signs (circling, nystagmus, rolling), and occasionally behavioral changes. Uveitis and cataracts may be present in young rabbits. Infected animals are usually in good flesh. Lesions are frequently confined to the kidney and appear as focal, irregular, depressed areas 1-100 mm in diameter. In severely affected

FIG. 6.57. Kidneys from a rabbit with chronic encephalitozoonosis. There are multiple, irregular pitted, and depressed regions of the renal cortex.
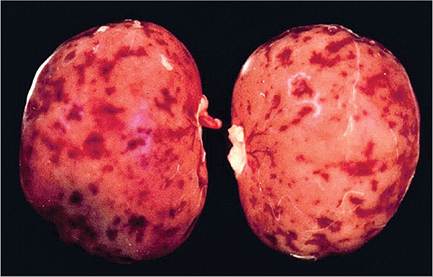
FIG. 6.58. Kidneys from a rabbit with recent Encephalitozoon infection. There are multiple irregular dark red and depressed foci of the renal cortex.
kidneys, lesions often coalesce with adjacent foci (Figs. 6.57 and 6.58). On cut surface, indistinct, linear, pale gray-white areas may extend into the underlying cortex.
On histopathology, granulomatous lesions may be evident in the interstitium of the lung, kidney, and liver. In the lung, focal to diffuse interstitial pneumonitis, with mononuclear cell infiltration, may occur. Hepatic lesions are characterized by a focal granulomatous inflammatory response (Fig. 6.59), with periportal lymphocytic infiltration. Focal lymphocytic infiltrates may also occur in the myocardium. In the kidney, early lesions consist of focal to segmental interstitial nephritis, with degeneration and sloughing of tubular epithelial cells (Fig. 6.60). Lesions may be present at all levels of the renal tubule, with minimal involvement of the glomeruli. Using tissue Gram stains, spores are evident as ovoid, Gram-positive organisms approximately 1.5 ? 2.5-5 μm in size. Staining procedures using carbol fuchsin will stain the organisms a distinct purple color. During early infection, spores may be present within epithelial cells, macrophages, inflammatory foci, or free within collecting tubules. In renal lesions of longer duration, interstitial fibrosis, collapse of the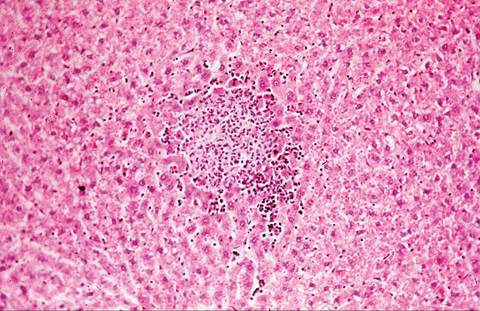
FIG. 6.59. Focal nonsuppurative hepatitis associated with disseminated Encephalitozoon infection.
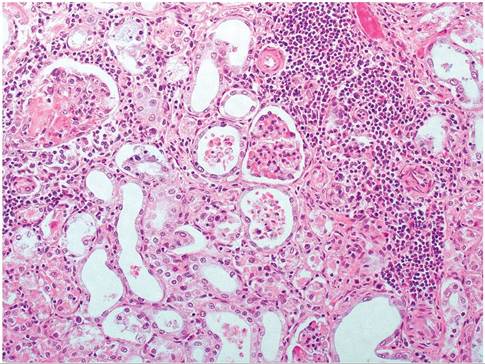
FIG. 6.60. Kidney from a rabbit with encephalitozoonosis. There is infiltration of the interstitium with mononuclear leukocytes, degeneration of tubular epithelium, and cellular debris within tubular lumina.
parenchyma, and mononuclear cell infiltration are typical changes, but the organism may no longer be detectable. When present, Gram-positive spores may be apparent in tubular epithelium or within tubular lumina (Fig. 6.61). In the central nervous system, lesions normally do not occur until at least 30 days postexposure. Changes include multifocal nonsuppurative meningitis and granulomatous encephalomyelitis, with astrogliosis and perivascular lymphocytic infiltration.
Pseudocysts filled with organisms may be apparent (Fig. 6.62). Using appropriate stains, pseudocysts containing organisms may be evident as collections of spores within parasitized astroglia or as scattered organisms within granulomatous inflammatory foci. These lesions may also be present in the central nervous system in the absence of identifiable organisms. Severe malacia associated with intense inflammation may rarely be observed,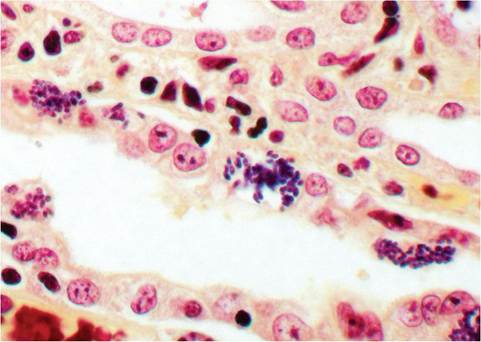
FIG. 6.61. Encephalitozoon spores within renal tubular epithelium and tubular lumen of a rabbit with chronic encephalitozoonosis (Brown and Brenn stain).
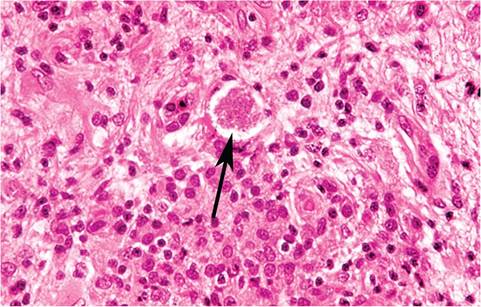
FIG. 6.62. Focal granulomatous encephalitis associated with chronic Encephalitozoon cuniculi infection. Note the pseudocyst containing organisms (arrow).
particularly in severely stressed or immunosuppressed rabbits. Lesions most frequently arise in the cerebrum, but may also occur in the brain stem, spinal cord, and cerebellum.
Phacoclastic uveitis (Fig. 6.63) and cataract formation (Fig. 6.64) occur in rabbits, and it is believed to follow transplacental infection. This syndrome is common among dwarf rabbits, but other breeds may be affected. On histological examination of the eye, keratitis, rupture of the lens capsule, and inflammatory cell infiltrates comprised of heterophils, foamy macrophages, and multinucleate giant cells are typical changes. The iris and ciliary body are infiltrated with lymphocytes and plasma cells. Using immunohistochemistry or tissue Gram stains, organisms may be identified, interspersed either around fragmented lens fibers or within macrophages.
Diagnosis
Identification of characteristic lesions and the demonstration of the organisms in tissue sections are the standard diagnostic procedures used to confirm the diagnosis. The organisms can be readily differentiated from protozoal infections, such as toxoplasmosis, by the

FIG.
6.63. Phacoclastic uveitis in a rabbit infected with Encephalitozoon cuniculi. (Courtesy A. Strom, Veterinary Ophthalmology Service, UC Davis School of Veterinary Medicine.)
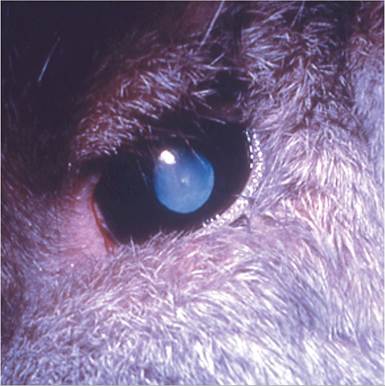
FIG. 6.64. Dwarf rabbit with a cataract associated with Encephalitozoon cuniculi infection. Some breeds of dwarf rabbits appear to be particularly susceptible to congenital E. cuniculi infection.
tissue tropisms and the staining properties of the organisms. Toxoplasma organisms are Gram-negative and do not stain with carbol fuchsin stains. An intradermal skin test has been used to detect infected rabbits, but serology has been the most widely used. Differential diagnoses for rabbits with neurologic signs include otitis interna, toxoplasmosis, and Baylisascaris migration.
More on the topic Encephalitozoon cuniculi Infection: Encephalitozoonosis; Microsporidiosis:
- Encephalitozoon cuniculi Infection: Microsporidiosis
- Encephalitozoon cuniculi Infection
- Treponema paraluis-cuniculi Infection:
- Psoroptes cuniculi Infestation: Psoroptic Mange; Ear Canker
- Demodex cuniculi Infestation: Demodectic Mange
- Picornavirus Infection: Mouse Encephalomyelitis Virus Infection
- Arenavirus Infection: Lymphocytic Choriomeningitis Virus Infection
- Arterivirus Infection: Lactate Dehydrogenase-Elevating Virus Infection
- Coronavirus Infection: Mouse Hepatitis Virus Infection
- Streptococcus pneumoniae Infection: Pneumococcal or Diplococcal Infection
- Giardia duodenalis Infection
- Malassezia spp. Infection: Malasseziasis