Streptococcus pneumoniae Infection: Pneumococcal or Diplococcal Infection
In the past, diplococcal (pneumococcal) infections due to S. pneumoniae were recognized to be a common problem in laboratory rats. Today, outbreaks of clinical disease are rarely recognized in well-managed, barrier- maintained facilities.
The organism is carried primarily in the nasoturbinates and tympanic bullae in clinically normal rats. Some of the serotypes isolated from rats are identical to those isolated from human cases, and human carriers have been implicated as a possible source of the organism. Conversely, S. pneumonia-infected rats represent a potential zoonotic hazard. Streptococcus pneumoniae may cause acute primary disease with mortality, but frequently it represents an important secondary invader, particularly in respiratory infections. An abundant polysaccharide capsule enables the organism to resist phagocytosis by the host cells. Pneumococci are not known to produce soluble toxins. However, several of the recognized serotypes produce tissue damage by activation of the alternate complement pathway. In clinically normal animals infected with the organism, predisposing factors such as concurrent infections or environmental changes may precipitate disease.Pathology
Clinical signs may include serosanguinous nasal discharge, rhinitis, sinusitis, conjunctivitis, and vestibular signs consistent with middle ear infection. At necropsy, there may be serous to mucopurulent exudate present in the nasal passages, with variable involvement of the tympanic bullae. In the acute systemic form of the disease, there are variable patterns of characteristic fibri- nopurulent polyserositis, including pleuritis, pericarditis (Fig. 2.43), peritonitis, periorchitis, and meningitis. Fibrinopurulent lesions may be confined to the lepto- meninges in some fatal cases. There may be consolidation of one or more lung lobes. Affected areas are dark red to dull tan and relatively firm and nonresilient.
On microscopic examination, in the acute form of the disease, fibrinopurulent pleuritis and pericarditis are typical findings. Pulmonary changes vary from localized suppurative bronchopneumonia to acute fibrinopurulent bronchopneumonia, with obliteration of the normal architecture in affected lobes. Fibrinopurulent peritonitis, perihepatitis, and/or leptomeningitis are frequent findings. Suppurative rhinitis and otitis media may also occur. Embolic suppurative lesions have been observed in organs such as liver, spleen, and kidney. In more chronic, localized disease states, pneumococcal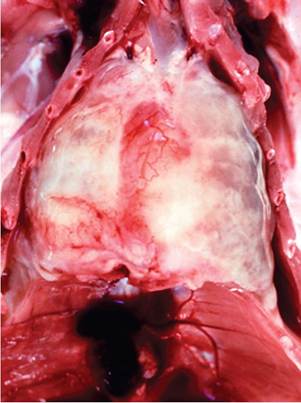
FIG. 2.43. Fibrinous pericarditis and pleuritis in a young rat with acute diplococcal (Streptococcus pneumoniae^ infection.
infections have been associated with suppurative bronchopneumonia in chronic respiratory disease, as well as otitis media.
Diagnosis
The presence of fibrinopurulent serositis is characteristic when present, and demonstration of the typical encapsulated diplococci in Gram-stained smears from lesions will provide a provisional diagnosis. Confirmation of streptococcosis requires the collection and culture of material from lesions and identification of the alpha- hemolytic organism. Nasal lavage at necropsy is a recommended procedure to recover the organism for bacterial culture. Differential diagnoses include cory- nebacteriosis, salmonellosis, pseudomoniasis, and pasteurellosis.
Bacterial PyelonephritisZNephritis
Suppurative pyelonephritis is more commonly encountered in male rats, and may be associated with a concurrent disease process, such as cystitis or prostatitis. A variety of bacteria have been recovered from affected kidneys, including Escherichia coli, Klebsiella sp., P. aeruginosa, Corynebacterium sp., Streptococcus sp., Enterococcus spp., and Proteus sp. The lower urinary tract is considered to be the most likely portal of entry in pyelonephritis. Excavation of the renal papilla, dilation of the renal pelves, and the accumulation of suppurative inflammatory exudates are typical findings. In cases of suppurative nephritis involving the renal interstitium, descending infections with bacterial emboli are the usual source of the infection. Streptococci are the most common isolates. Lesions are similar to those seen in other species with suppurative disease processes of this system.
More on the topic Streptococcus pneumoniae Infection: Pneumococcal or Diplococcal Infection:
- Klebsiella pneumoniae Infection
- Picornavirus Infection: Mouse Encephalomyelitis Virus Infection
- Arenavirus Infection: Lymphocytic Choriomeningitis Virus Infection
- Arterivirus Infection: Lactate Dehydrogenase-Elevating Virus Infection
- Coronavirus Infection: Mouse Hepatitis Virus Infection
- PNEUMOCOCCAL INFECTIONS
- Chlamydophlla spp. Infection
- INFLAMMATION IN HIV-1 INFECTION
- Blastomyces dermatitidis Infection
- Mycobacterium Avium Complex Infection
- Characteristics of Infection and Disease
- Astrovirus Infection
- COVID-19 INFECTION
- IN HIV-1 INFECTION
- Monitoring HIV infection
- Pathogenesis and Stages of MAP Infection in Cattle