Microscopic Detection of M. bovis
The use of microscopy to detect acid-fast bacteria (AFB) is a rapid and inexpensive, but inconclusive, method to tentatively diagnose mycobacterial infections. The presence of AFBs justifies a presumptive diagnosis of tuberculosis, especially when clinical signs and typical lesions are present.
Microscopic examination can be done in two main ways: firstly, by examining smears from mucus obtained from the respiratory tract, or smears prepared from exudate obtained from lesions resembling those caused by M. bovis and, secondly, by detecting AFBs in histological sections of tissues containing the suspect lesions.Smear Examination Conventionally, smears for TB diagnosis are stained with the Ziehl-Neelsen (ZN) technique that allows detection of acid-fast bacteria (AFB) (Fig. 9.30), but auramine O/rhodamine staining and immunohistochemistry are also used (Varello et al. 2008), the latter of which is the most sensitive (Watrelot- Virieux et al. 2006). The smears, except those made from respiratory mucus, should be made from exudate obtained from visible tuberculous lesions. In the case of histopathology, tissue specimens from a portion of the lesion bordering normal tissue, should be fixed in 10% buffered formalin for processing. The biggest limitation of using this technique is that the specific mycobacterial genus cannot be determined, and mycobacteria can also morphologically be confused with Rhodococcus equi that is also acid-fast. Generally, smear examination is very specific, but it has a low Se because smears from fresh specimens require up to 10,000 bacteria/ml for smear positivity, and not all cases with tuberculosis are shedders (Adu-Bobi et al. 2009). For ZN-stained smears the Se and Sp were, respectively, 33.9 and 100% (Varello et al. 2008), while Damina et al. (2011) recorded a Se of 82.7%. Not all investigators reported the same results, as in Burkina Faso, Tarnagda et al.
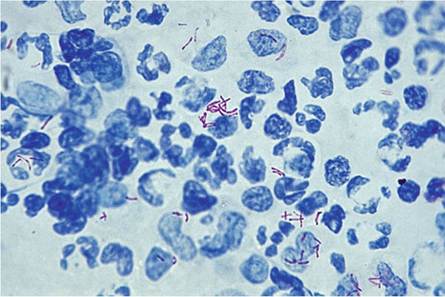
(2014) detected AFBs in only 37.3% of smears prepared from 102 animals with BTB-like lesions.Fig. 9.30 Microscopical appearance of a positive, Ziehl-Neelsen-stained smear of exudate collected from a tuberculous lesion containing scattered, and a small cluster of acid-fast mycobacteria (1000 x magnification)
Smears from nasal or respiratory tract mucus are not often used in animals, but they have been used, for instance, to diagnose TB in elephants (Mikota et al. 2001) and recently in lions (Miller et al. 2015). Smear examination is not considered to be a reliable diagnostic technique and it has a low Se and Sp. In wildlife, the use of microscopy has been recommended for surveys and game meat inspection, particularly when combined with macroscopic postmortal examination (Maas et al. 2013). Histopathology The examination of histological sections for diagnosing BTB is not a stand-alone test. It should be used to confirm a macroscopical presumptive diagnosis based on the presence of lesions resembling those expected in animals suffering from BTB. In histopathological sections, the diagnosis is based on the presence of the typical appearance of the lesion, in addition to the presence of AFBs, or those stained with auramine O, or by immunocytochemistry. Depending on the species of animal, and the nature of the lesion, very few bacteria may be present (paucibacillary cases), or they may not be visible at all, probably because of their limited numbers in the exudate. Not being able to detect AFBs histologically is not a reason to rule out M. bovis as the cause of the lesion, as is the case with smears, when there are too few bacteria in the lesions to allow their detection. This is a known phenomenon in many species, including wildlife, and particularly in African buffaloes, where a large percentage of cases with lesions do not contain detectable bacteria histologically.
The Se and Sp of the technique tend to differ in various published studies. Varello et al. (2008) found a high Se (93.4%) and Sp (92.3%) for histopathology, but it is clear that postmortal inspection, histopathology, and culture do not detect the same sets of positive animals, although there is an overlap between the results of the individual tests. Using these tests in series or in parallel increases the Se (Rohonczy et al. 1996). The use of PCR to identify the different MTC species on histological sections also increases the sensitivity of the investigation in those cases where histopathology reveals typical tuberculous lesions and the presence of mycobacteria, but the specimens were culture negative (Miller et al. 2002).
9.8
More on the topic Microscopic Detection of M. bovis:
- Microscopic Polyangiitis
- Detection, Investigation and Preparation
- HEAT DETECTION
- PREGNANCY DETECTION
- Detection of MAP in Crohn’s Disease Patients
- DETECTION OF DNA FRAGMENTATION
- Extensive neuropathologic studies have demonstrated that neural tube defects are associated with a high incidence of gross and microscopic malformations of the forebrain and hindbrain (34).
- Zoonotic (M. bovis) TB in Humans in Cameroon
- Mycobacterium bovis Infection in Humans
- Prey exhibit behaviors that can prevent detection or deter predators
- Public Heath Implication of M. bovis
- Human TB Due to M. bovis
- Inferences on the Origin of M. bovis
- Tuberculosis Caused by M. bovis in Humans in Uganda
- 5.3 Maintenance Hosts of Mycobacterium bovis
- Corynebacterium bovis Infection: Coryneform Hyperkeratosis; Scaly Skin Disease
- Genetic Diversity of Mycobacterium bovis Strains in Tanzania