Abnormal Cytology
Malassezia
Malassezia spp. can be found on cytology from up to 96% of dogs and 83% of cats with normal ear canals.10 Malassezia pachydermatis is widely recognized as the predominant commensal yeast of dogs.12-15 However, the genus actually consists of eight species, including seven distinct lipid-dependent species: M.
furfur, M. sympodialis, M. globosa, M. obtusa, M. restricta, M. sloofiae, and M. equi.12,13 In dogs with otitis externa, Malassezia pachydermatis is present 83% of the time.16-18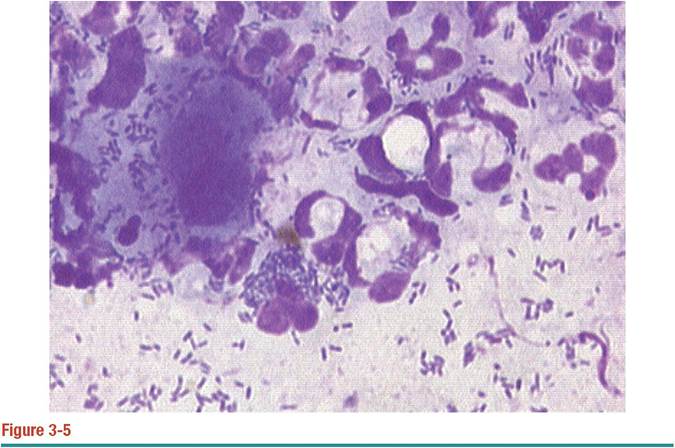
Cytology from severe bacterial otitis with Pseudomonas aeruginosa. Numerous polymorphonuclear neutrophils are present. Rod bacteria can be seen intracellularly (phagocytosis) and extracellularly.
Recent studies have demonstrated M. furfur and M. obtusa in 4.5% of cases of canine otitis externa, whereas M. sympodialis and M. furfur were present in 8.9% of diseased ear canals of cats.18,19 M. sympodialis,20,21 M. globosa,21 and M. furfur18,21 can be recovered from normal-haired skin, ear canals, and mucosa of healthy cats. Of these, M. sympodialis is believed to be a normal resident of the feline ear canal.15
Because the different species may have variable morphologic features and staining characteristics, veterinarians may notice unusually shaped yeast bodies on cytologic preparations. Most likely these variations represent multiple species of Malassezia. Current research demonstrates that different species have variable pathogenicity, virulence factors, and host responses; however, the clinical relevance of these differences has not been demonstrated.13 Unless there is a compelling reason to differentiate between Malassezia species using laboratory techniques, cytologic recognition of any member of the genus is sufficient for management of clinical cases.
Because Malassezia can be found in normal patients or mixed in with predominantly bacterial infections, veterinarians need to determine the clinical significance of Malassezia for each patient. Cytology is the most useful tool for differentiating between normal resident colonization and overgrowth. Unlike bacterial infections, suppurative inflammation is not a common feature of Malassezia otitis5 and therefore cannot be used to determine a pathologic state.
At what threshold does yeast become a contributing factor to disease rather than an incidental finding? Precise breakpoints for maximum acceptable number of yeast vary from patient to patient. Cytologic estimation of numbers can provide a guideline for the clinician; in the end, however, the decision to treat Malassezia depends on a combination of cytologic findings, severity of clinical signs, past history of yeast otitis, and response to previous therapy in that individual patient. A recent comparison of cytologic specimens from normal and diseased ears demonstrated that up to an average of two yeast per high-dry field (40? objective, 400? magnification) in the dog and cat should be considered normal.22 Mean counts greater than 5 yeast per field in dogs, and 12 yeast per field in cats are abnormal. Intermediate values are considered a gray zone (Table 3-1). These criteria had a specificity of 95% in dogs and 100% in cats. However, because the study included bacterial otitis, not all cases of otitis externa had yeast as a component; as a result, sensitivity was only 50% for
TABLE 3-1 Recommended Breakpoints for Numbers of Organisms Identified Cytologically. Reported as Mean Number of Organisms per High-Dry Field (40? Objective)
| NORMAL | INTERMEDIATE | ABNORMAL | |
| Malassezia | |||
| Dog | ≤2 | 3-4 | ≥5 |
| Cat | ≤2 | 3-11 | ≥12 |
| Bacteria | |||
| Dog | ≤5 | 6-24 | ≥25 |
| Cat | ≤4 | 5-14 | ≥15 |
dogs and 63% for cats.
A study by Tater et al10 evaluated otic cytology from 50 normal dogs and 52 normal cats; it found a range of 0 to 2.6 yeast per high-dry field in dogs and 0 to 3.3 per high-dry field in cats. Diseased dogs were not included for comparison, but these findings would be consistent with previously reported normal breakpoints. The authors also demonstrated that ear conformation did not result in differences in normal yeast numbers when comparing dogs with pendulous pinna with dogs with erect ear carriage. Therefore, ear conformation should not influence interpretation of cytologic findings.Malassezia may also colonize the tympanic cavity, causing or contributing to otitis media. In one study, Malassezia was recovered from 65.8% of external ear canals and 34.2% of middle ears of dogs with chronic otitis.8 Yeast can be found mixed with bacteria; however, in the study by Cole et al,8 23.7% of dogs had otitis media associated with Malassezia infection alone. Malassezia is not a normal resident of the tympanic cavity; therefore, any finding on cytology from this space is considered abnormal, and systemic antifungal therapy is indicated.
Candida
Candida albicans is a normal resident of the skin and gastrointestinal (GI) tract of dogs and cats. Under appropriate circumstances, Candida can become an opportunistic pathogen. Compared with Malassezia, Candida spp. are not common pathogens in cases of otitis externa. In a study by Ginel et al,22 three of 24 dogs (12.5%), and two of 22 cats (9.1%) with clinical signs of otitis externa had cytologic and culture evidence of Candida spp. Cytologically, Candida are thin-walled, round to oval, and approximately 2 to 6 μm in diameter.23 A thin, clear capsule displaces stain and sediment, giving the appearance of a halo around the yeast body. The organism exhibits narrow-based budding and can form short, tubular, septate pseudohyphae. In contrast, Malassezia is unencapsulated, has broad-based budding, and never forms pseudohyphae or hyphae.
Bacteria
One of the primary uses of otic cytology is detection of the presence of bacteria. Unlike yeast, which can be readily identified using the 40? objective, proper evaluation for bacteria requires high magnification with an oil-immersion lens (100? objective, 1000? magnification). The diameter of most coccoid bacteria is typically 0.3 μm; coliform, rod bacteria are typically less than 1.5 μm in length.24 In spite of this small size, and given quality equipment and practiced skill and ability, cytology can actually be more sensitive than culture for detecting bacteria.5,10 In one study of normal ear cytology, gram-positive cocci were identified in 42% of dogs by cytology but only 25% by culture. The actual percentage of normal patients with cytologic or culture evidence of bacteria may vary significantly based on geographic location and humidity. Ear conformation has not been shown to influence cytologic findings.10
Determining the significance of bacteria seen on cytology depends on several factors: morphology, numbers, and concurrent leukocytes. After bacteria have been identified, the clinician should determine whether there is a monoculture of a single morphologic type or whether a mixed infection is present, and then describe the morphology of bacteria seen. The presence of larger cocci arranged in pairs or tetrads is typical morphology for Staphylococcus spp; small cocci in short chains are characteristic of Streptococcus and Enterococcus spp. Even with these guidelines, laboratory culture is necessary to make a definitive speciation; clinicians should record findings as pairs of cocci or chains of cocci rather than attempt to make a specific diagnosis based on cytology. Corynebacterium is a large plump rod that may be found in normal or diseased ears. The most common rod-shaped pathogens associated with otitis externa are Pseudomonas spp. and Proteus spp. In tropical climates, coliform bacteria may be considered a normal finding.
In more arid regions, only gram-positive cocci are commonly observed in normal patients.In addition to morphology, the number of bacteria present should be estimated for each case. A semiquantitative cytologic criteria, similar to that proposed for Malassezia, can be used for bacteria (see Table 3-1). Based on the results reported by Ginel et al,22 fewer than five bacteria per high-powered dry field (40? objective) should be considered normal; more than 25 bacteria per field supports the diagnosis of an abnormally increased population. Using higher magnification, fewer than two bacteria per high-oil field (100? objective) is normal, and more than 10 bacteria per field is abnormal. For cats, fewer than four bacteria per 40? field (1.6 per 100? field) was consistent with normal conditions, and more than 15 bacteria per 40? field (6 per 100? field) was abnormal. Intermediate numbers in a gray zone are subject to interpretation. Using these mean-count breakpoints to differentiate normal from diseased ears yielded 95% specificity and 50% sensitivity in dogs, and 100% specificity and 63% sensitivity for cats.
An important concept in determining the clinical significance of bacteria seen on cytology is the distinction between bacterial “overgrowth” and bacterial “infection.” In general, overgrowth refers to increased numbers of resident bacteria in the debris and on the epithelial surface of the external canal. Overgrowth may contribute to disease through the production of exotoxins that perpetuate inflammation; however, overgrowth does not typically warrant culture and susceptibility testing or expensive systemic therapy. In these cases, systemic therapy may be less effective than topical medications because the concentration of antibiotic achieved by topical medications can far exceed that achievable by systemic routes. Overgrowth can usually be managed effectively by frequent flushing, antiinflammatory therapy, and topical antibiotics directed at the specific organism(s).
Bacterial infections typically describe cases with purulent response to bacteria, ulceration of epithelial lining, or colonization of the tympanic cavity. These cases often require high-dose, long-term systemic antibiotic therapy for successful resolution.The most direct evidence supporting a diagnosis of infection instead of overgrowth is the presence of neutrophils on cytology. Leukocytes are not found in the normal ear canal. Bacterial overgrowth on surface debris rarely elicits the same neutrophilic response as bacterial infection of the external canal or tympanic cavity. The finding of bacteria within neutrophils (phagocytosis) strongly supports a diagnosis of infection with a significant bacterium.
Cytology, however, is not the only test that should be performed when evaluating bacterial otitis externa. Although cytology can demonstrate the presence, number, and relative significance of cocci or rods, it cannot be used to determine the species of bacteria. Bacterial culture is performed to identify species and determine the antimicrobial susceptibility of clinically relevant bacteria. Because culture does not differentiate between normal resident bacteria, bacterial overgrowth, and bacterial infection, cytology is the best tool to determine the relative significance of bacteria present in the external canal. Similarly, because culture does not accurately evaluate changes in numbers or the presence or absence of neutrophils, sequential bacterial cultures are not useful for monitoring response to therapy. Cytology is necessary to determine whether numbers of organisms are decreasing, if there is a change in the predominant organism, or if there is a change in the presence or absence of neutrophils. Bacterial culture in the absence of cytology is an inaccurate tool (Table 3-2).
When evaluating otitis media, a separate cytology should be performed from the tympanic cavity. Veterinarians should not assume that the same organism contaminates both sites. In a study comparing isolates from the horizontal canal and the tympanic cavity of dogs with chronic otitis externa and media, differences were noted in the species or antimicrobial susceptibility of bacteria isolated in 89.5% of the cases.8 Therefore, samples for cytology and culture should be obtained from the tympanic cavity rather than the external canal.
Leukocytes
Unlike bacteria and yeast, which may be found in the normal ear canal, white blood cells are only present in cytologic specimens from abnormal ears. Leukocytes enter the ear canal as the result of exocytosis across severely inflamed epithelial lining, through ulceration of epithelial lining, or by extension from the tympanic cavity during otitis media. Therefore, practitioners should always examine slides carefully for white blood cells, in addition to bacteria and yeast, and document the findings in the medical record.
TABLE 3-2 Comparison of Cytology and Culture for Evaluation of Otitis Externa
| ATTRIBUTE | CYTOLOGY | CULTURE |
| Time to available results | Immediate | 48-72 hours |
| Sensitivity for yeast | High | Low |
| Sensitivity for bacteria | High | Moderate to high |
| Sensitivity for leukocytes | High | None |
| Estimation of numbers | Semiquantitative | Categorical data |
| Rank significance in mixed infection | Yes | No |
| Monitor response to therapy | Yes | No |
| Detection of antimicrobial resistance | No | Yes |
Because neutrophils rarely respond to bacterial overgrowth in debris, the presence or absence of neutrophils is a reliable tool for differentiating overgrowth from true infection. Phagocytosis of bacteria is also worth noting, particularly in mixed infections; the organism being targeted is more likely the significant pathogen compared with bacteria free in the background. Extension of purulent exudate from the middle ear to the external canal may be the only evidence readily available to clinicians that a concurrent otitis media is present in a dog presenting for otitis externa. Because otitis media is present in 16% of dogs with acute otitis externa and up to 82% of dogs with chronic disease,6,8 any cytologic evidence of leukocytes in the external canal should increase the clinician’s suspicion for concurrent otitis media, warranting specific diagnostic evaluation. As a general rule, if the patient’s body is responding to an infection with suppurative or pyogranulomatous inflammation, systemic antibiotic therapy is almost always indicated. Whenever appropriate, a culture and susceptibility should be obtained to modify empirical antibiotic selection; in the case of otitis media the sample should be obtained directly from the tympanic cavity.
The presence or absence of leukocytes on cytology is a useful tool for monitoring the progression of disease or response to therapy. Progression from otitis externa to otitis media, or progression from Malassezia otitis or bacterial overgrowth to bacterial infection should not be missed due to failure to perform and document otic cytology. When monitoring therapy in a difficult case of Pseudomonas otitis, the disappearance of leukocytes during the first recheck is a strong indication of improvement even if small numbers of bacteria remain; in contrast, bacterial culture would simply identify Pseudomonas on both visits, leading the veterinarian to believe the case was not responding adequately. A serial cytologic record from each episode helps veterinarians avoid inappropriate therapeutic decisions.
Parasites
Heat-fixed, stained cytologic specimens from otic debris will occasionally contain evidence of parasites, but direct mineral-oil preparation is a more reliable method for specific parasite evaluation. Low-magnification (4? objective) microscopic examination of a mineral-oil preparation is sufficient for identifying ear mites. In all cases the presence of any insect or mite in the external ear canal is considered abnormal and should be pursued accordingly.
In both dogs and cats the most common parasite associated with otitis externa is Otodectes cynotis.6,1,25 When large numbers of mites are present in the external ear canal, the diagnosis can be easily confirmed by direct visualization of the mites with a magnified operating-head otoscope or video otoscope. O. cynotis has a psoropti- form body type, similar to Sarcoptes, but is larger and has short, unjointed pedicles extending from the legs. The larger adult female mite is approximately 280 μm wide and 450 μm long26; the rudimentary fourth pair of legs does not extend beyond the body. The slightly smaller adult males (250 ? 320 μm) are frequently observed attached to eight-legged deutonymphs (220 ? 320 μm). Other life stages include the protonymph (160 ? 240 μm) and six-legged larva (115 ? 240 μm). Numerous large eggs (100 ? 210 μm) are commonly found lodged in the keratin debris. Identification of a single egg or mite of any life stage provides a definitive diagnosis. However, ear mites cannot be ruled out by the absence of O. cynotis on microscopic evaluation. A treatment trial with appropriate miticidal therapy is strongly recommended for all cases of chronic otitis externa.
Other mites occasionally found on cytologic preparations include Demodex spp., Sarcoptes scabiei, Notoedres cati, Eutrombicula alfreddugesi, and Neotrombicula autumnalis.
Demodex, the follicular mange mites of dogs and cats, can colonize any hair follicle, including those of the external ear canal. In normal dogs, Demodex rarely causes any significant problems; however, in patients with juvenile-onset or adult-onset demo- dicosis, overpopulation and colonization of hair follicles of the ear canal may cause secondary bacterial infections, folliculitis, furunculosis, inflammation, and edema, resulting in clinical otitis externa. Although Demodex is considered a normal resident organism, these mites are very rarely found in ear cytology from normal dogs. Therefore, if Demodex mites are found on microscopic evaluation of otic exudate, demodicosis should be suspected, and a thorough examination and skin scrapings of multiple regions of haired skin are indicated.
Sarcoptes scabiei and Notoedres cati, the sarcoptic mange mites of cats, most commonly affect the host’s pinna, rarely causing inflammation of the external canal. Chiggers, or harvest mites, Eutrombicula alfreddugesi, and Neotrombicula autum- nalis cause pruritus, papules, erythema, and crusting where they attach to the skin. Occasionally the parasitic larval stage is found tightly adhered to the skin around the entrance to the external ear canal. The large (500 μm), six-legged larvae are easily distinguished from Otodectes cynotis by their different body type and bright red- orange color.
Neoplasia
Although not common, the external ear canal can be a site for development of many different types of neoplastic and non-neoplastic masses. Symptoms of masses in the ear canal such as otorrhea, head shaking, and malodor are similar to presenting signs for other causes of otitis. The presence of secondary bacterial or yeast infections and subsequent debris may also obscure the actual cause of disease. Not all tumors exfoliate on normal cytology, but the finding of large sheets of epithelial cells is one cytologic finding that should always prompt further investigation for neoplasia.
Any nodule found in the external canal should be evaluated for neoplastic potential. Under sedation, cytologic samples can be obtained by fine-needle aspirate or curettage. Fine-needle aspirate is most useful for masses easily visible in the vertical canal. For nodules in the horizontal canal, curettage can be performed through an otoscopic cone, with one hand holding the otoscope and the other manipulating a sharp-edged curette. The curette is positioned over or just beyond the tumor and then angled and dragged back across the surface. The cells collected are spread gently across two or three glass slides and allowed to air dry prior to staining; heat fixing is not recommended because this will distort cellular features. Occasionally small tumors may be removed and submitted for histopathology by this method; for larger tumors the goal is to differentiate inflammatory hyperplasia, benign neoplasia, and malignant neoplasia.
If the predominant cell type is inflammatory, appropriate antiinflammatory therapy can be prescribed, followed by reevaluation. Sheets or clusters of large round cells may be indicative of an epithelial tumor such as ceruminous gland adenoma or adenocarcinoma, squamous cell carcinoma, basal cell tumor, lymphoma, histiocytoma, or plasmacytoma. Spindle-shaped cells may represent fibrosis of the canal, fibrosarcoma, or other nonepithelial tumor. Mast cells are more easily recognizable. Cytology from nasopharyngeal polyps may be characterized by epithelial cells with visible respiratory cilia at one margin. If cytologic evaluation is uncertain or the cytologist is concerned about either epithelial or nonepithelial tumors, specimens should be submitted for laboratory evaluation by a clinical pathologist and an incisional biopsy for histopathology should be obtained to confirm the diagnosis.
Conclusion
Cytology is a simple, rapid, and practical diagnostic test that should be performed routinely for every patient with clinical signs of otitis externa. Cytologic specimens should be evaluated for the presence, numbers, and characteristics of three key features: yeast, bacteria, and leukocytes. More than five yeast or 25 bacteria per high-powered field is suggestive of significant microbial activity, warranting therapeutic intervention. The presence of white blood cells on cytology indicates true infection, warranting systemic therapy, as opposed to bacterial overgrowth in debris, which can often be managed successfully with topical therapy. Cytology improves all aspects of case management, including diagnosis of secondary infections, monitoring progression of disease, and evaluating response to therapy.
More on the topic Abnormal Cytology:
- Normal Cytology
- Cytology
- Cytology and Histopatnology of the Ear in Health and Disease
- Abnormal Bony Density or Structure
- Abnormal Findings
- Abnormal Radiographic Findings
- Description and Pathophysiology of the ART-Related Abnormal Fat Distribution
- Instrumented gait analysis has evolved into a recognized objective evaluation that is important in surgical and rehabilitation therapy planning for the child with an abnormal walking pattern.
- Rheumatic disorders (connective tissue disorders or collagen vascular disorders') is a collective term to denote a large group of conditions with variable manifestations but two common characteristics: (a) acute or chronic inflammation of multiple target organs, specially musculoskeletal system and vasculitis, and (b) an underlying abnormal immune response, e.g. autoimmune etiology.
- Index
- Specific Strategies for Successfully Marketing Preventive and Therapeutic Ear Care
- PRION DISEASES
- Histopathology
- Hepatitis and cholestasis
- Barbering and Trichotillomania
- PATHOLOGY
- DISORDERS OF ORBIT
- VISION DISORDERS
- HIGH-RISK NEWBORN
- Evaluation of the Patient With Renal Disease