Mycoplasma pulmonis Infection: Murine Respiratory Mycoplasmosis
Chronic respiratory disease in rats has undergone an interesting historical evolution. Initially believed to be multifactorial, it later became apparent that M. pulmonis could be the primary pathogen in this disease.
This gave rise to the term murine respiratory mycoplasmosis (MRM) as the preferred terminology over CRD. However, other pathogens of the respiratory tract were shown to play a role in CRD, including CAR bacillus, respiratory viruses, and environmental factors, thereby returning the term CRD as the most appropriate and inclusive moniker for this disease. Nevertheless, M. pulmonis remains the major pathogen in cases of CRD. Mycoplasma pulmonis is a member of the order Mycoplasmatales, small pleomorphic bacteria devoid of cell walls that have specialized tip structures that play a key role in attachment to host cells. Respiratory disease results from loss of cilia following colonization of respiratory epithelium (Fig. 2.21). Some antigenic heterogeneity occurs among strains of M. pulmonis. There are demonstrable common cross-reactive antigens among 2 other naturally occurring murine mycoplasmas, M. neurolyticum (mice) and M. arthritidis, but M. pulmonis is the only clinically significant Mycoplasma sp. in rodents.Epizootiology and Pathogenesis
Quality control programs in laboratory animal medicine have resulted in a marked reduction in the incidence of
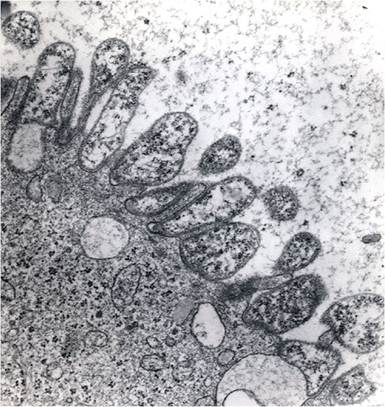
FIG. 2.21. Electron micrograph of bronchiolar epithelium heavily colonized with Mycoplasma pulmonis, resulting in complete loss ofcilia.
myocoplasmosis in rats. However, based on serological surveys, seropositive colonies continue to be identified, and infection in wild and pet rats is common. Transmission of M. pulmonis among cage-mates and to adjacent cages occurs inefficiently by aerosols.
It may require up to several months to establish an infection in contact animals, and clinical disease may not occur until up to 6 months after infection. Intrauterine transmission may also occur, although newborn pups appear to be frequently infected by exposure to the infected dam during the postnatal period. Placentitis and fetal bronchopneumonia have been produced in pregnant rats inoculated intravaginally with M. pulmonis prior to breeding. The incidence and intensity of the disease are influenced by a variety of factors, such as strain of rat, concurrent infections, and environmental conditions. For example, LEW rats develop a more severe disease than do F344 rats. Concurrent infections with organisms, such as Sendai virus, rat coronavirus, or CAR bacillus, have an additive effect on CRD. Similarly, other opportunistic secondary bacterial invaders frequently play a role in the progression of the disease. Ammonia concentrations at the cage level of greater than 25 ppm may enhance the progression of CRD.Mycoplasma pulmonis has an affinity for respiratory epithelium, middle ear, endometrium, and less commonly, synovium. Invasion of the middle ear probably occurs via the Eustachian tube. This usually results in a chronic otitis media, since the Eustachian tube opens into the tympanic bulla on the dorsal aspect, affording poor drainage to the nasopharynx. Colonization of respiratory epithelium results in ciliostasis, with resulting impaired airway clearance and accumulation of lysozyme-rich inflammatory exudate. Since intrapulmonary airways lack cartilage, bronchioles are subject to bronchiolar expansion and bronchiolectasis. Host cell damage may occur by a variety of means including uptake of essential cell metabolites and release of cytotoxic substances such as H2O2. Both the intact organisms and the cell membranes are nonspecific B-cell mitogens, resulting in marked peribronchiolar lymphocytic infiltration, which is a hallmark of CRD in the rat.
Pathology
Clinical signs vary, including subclinical infections, but can include minimal to florid respiratory distress, sniffling, torticollis, infertility, and arthritis. In severely affected animals, dyspnea, ruffled hair coat, and weight loss may occur. Porphyrin-containing dark red encrustations may be present around the eyes and external nares. At necropsy, serous to catarrhal exudate may be present in the nasal passages, trachea, and major airways. In animals with profuse viscid exudate in the airways, there may be patchy vesicular to bullous emphysema in the lungs. Early pulmonary lesions are usually manifested as pinpoint gray lesions. As peripheral bronchiolectasis becomes apparent, varying sized foci are present with clear mucous- or pus-filled lumina. Affected lobes and areas are usually cranioventral in distribution, unilateral or bilateral, often asymmetric in severity, and dark plumcolored to light tan (Fig. 2.22). One or both tympanic bullae may contain serous to inspissated purulent material, with thickening of the tympanic membrane. The uterine horns, ovarian bursae, and oviducts may contain purulent exudate, but involvement of these sites may only be confirmed microscopically. Disseminated
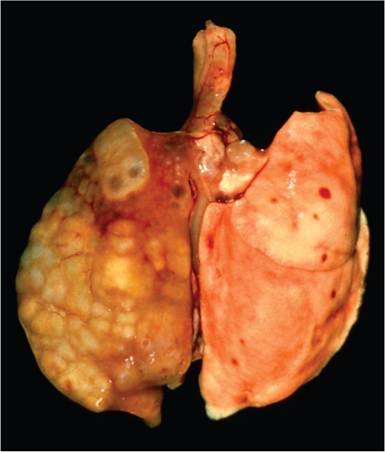
FIG. 2.22. Chronic respiratory disease in a rat associated with Mycoplasma pulmonis infection. Note the asymmetric involvement of lung lobes and the irregular surface of affected areas due to bronchiolectasis and peribronchiolar lymphocytic infiltration.

FIG. 2.23. Bilateral swelling of tibiotarsal joints in a young rat with
naturally acquired systemic Mycoplasma pulmonis infection. Arthritis is a rare component of mycoplasmosis in the rat.
infection may occasionally result in arthritis, with swelling of the tibiotarsus (Fig. 2.23).
Microscopic changes in the affected tympanic bullae, turbinates, and major airways are characterized by a leukocytic infiltrate in the submucosa consisting of neutrophils, lymphocytes, and plasma cells.
Epithelial cells in affected areas are often cuboidal to squamous, with loss of cilia, and hyperplasia of goblet cells. Leukocytes, mucus, and cell debris are frequently present on the surface in affected areas. Peribronchial, peribronchiolar, and perivascular infiltration with lymphocytes and plasma cells is a prominent feature at all stages of CRD (Fig. 2.24). Chronic bronchitis and bronchiolitis frequently progress to bronchiolectasis, characterized by dilation of airways, rupture of airways, and abscessation (Fig. 2.25). Collections of mucus, leukocytes, and cellular debris are present in the lumen (Fig. 2.26). There may be rupture of the bronchiolar walls, with release of inflammatory cells, mucus, and debris into the adjacent parenchyma and abscessation. Alveolar changes are often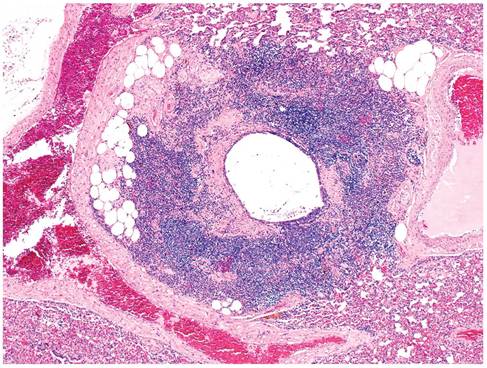
FIG. 2.24. Peribronchiolar cuffing with lymphocytes and plasma cells, a characteristic feature of Mycoplasma pulmonis infection in rats.
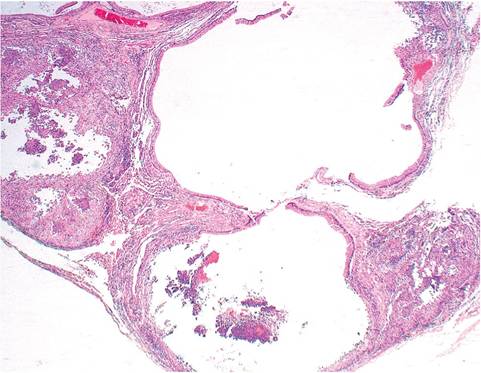
FIG. 2.25. Pulmonary lesions associated with an advanced case of mycoplasmosis. There is marked bronchiolectasis, rupture of airways, and abscessation.
focal to segmental in distribution. Macrophages, neutrophils, and mucus may be present in alveolar spaces, with lymphocytic infiltration in the alveolar septa. There may be variable degrees of alveolar emphysema, with focal to patchy rupture of alveolar septa. Genital tract lesions, when present, consist of perioophoritis and endometritis, with mononuclear and polymorphonuclear cell infiltration in the stratum compactum and endometrium. In some cases, the lumen may be packed with leukocytes. Inflammatory lesions may also arise in the male genital tract.
Diagnosis
CRD caused by M. pulmonis, CAR bacillus, or both has similar macroscopic and microscopic features. The role of CAR bacillus can be confirmed as already described.
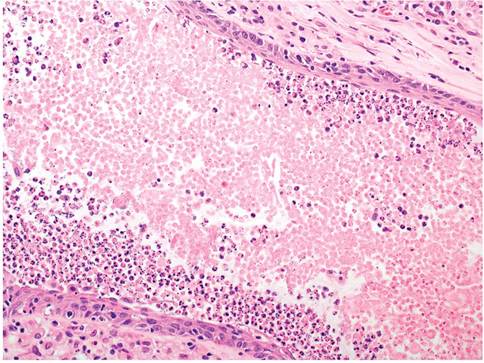
FIG. 2.26. Chronic bronchiolitis associated with murine respiratory mycoplasmosis. Note the squamous metaplasia of respiratory epithelium, loss of cilia, and necrotic cellular debris filling the lumen.
Mycoplasma organisms are not readily visible microscopically, but their presence may be inferred by lack of cilia on respiratory epithelium. Mycoplasma pulmonis can usually be cultured from nasopharyngeal washes or affected sites such as the upper and lower respiratory tract and uterus using appropriate media, and can also be detected by PCR or immunohistochemistry. Cultures may fail to detect the organism in some infected animals. Serology is commonly used for surveillance within a population. However, animals may be falsely seropositive due to exposure to M. arthritidis. In addition, rats naturally exposed to M. pulmonis may be seronegative for up to 4 months postexposure. Thus, there are limitations to relying solely on serology to confirm the diagnosis. The collection of tissues and sera from retired breeders is recommended as a useful means of screening for mycoplasmal infections. Serological testing for antibodies against coinfecting respiratory viruses such as Sendai virus, PVM, and rat coronavirus are recommended, particularly when lower respiratory disease is severe. These agents can have an additive effect on the progression of CRD. Cultures for conventional bacteria are critical, since there may be concurrent infections with other bacteria, such as Pasteurella pneumotropica or Streptococcus pneumoniae. Infection should be considered chronic, with no merit in antibiotic treatment other than palliating clinical signs. Differential diagnoses include pulmonary abscessation due to Corynebacterium kutscheri infection, chronic respiratory infections due to the CAR bacillus, otitis media due to conventional bacteria, and suppurative metritis due to P. pneumotropica infection.
More on the topic Mycoplasma pulmonis Infection: Murine Respiratory Mycoplasmosis:
- Cilia-Associated Respiratory Bacillus Infection
- Mycoplasma spp. Infections
- Murine Urologic Syndrome (MUS)
- OTHER MYCOPLASMA INFECTIONS
- Hemotropic Mycoplasma Infections
- 10.33 MALARIA MYCOPLASMA INFECTIONS
- MYCOPLASMA INFECTIONS OF AQUATIC MAMMALS
- CHAPTER 29 MYCOPLASMA INFECTIONS
- RESPIRATORY DISEASES
- D/D RESPIRATORY DISTRESS
- Respiratory Disorders
- Respiratory Failure
- RESPIRATORY DISTRESS
- CLINICAL EVALUATION OF RESPIRATORY DISEASE
- COMMON RESPIRATORY PROBLEMS
- RESPIRATORY FUNCTION
- Respiratory System
- ACUTE RESPIRATORY FAILURE
- Arterivirus Infection: Lactate Dehydrogenase-Elevating Virus Infection
- Contribution of Respiratory Dysfunction to Speech Disorders